Appearance
❓:In triangle ABC, AB = b^2 - 1, BC = a^2, CA = 2a, where a, b are integers greater than 1. Find b - a.
🧠:[<think>Okay, so I have this triangle ABC where the sides are given in terms of a and b. Specifically, AB is b squared minus 1, BC is a squared, and CA is 2a. Both a and b are integers greater than 1. I need to find the value of b minus a. Hmm, let's see.First, I remember that in any triangle, the sum of any two sides has to be greater than the third side. This is called the triangle inequality theorem. So, maybe I can use that to set up some inequalities here. Let me note down the sides again to be clear:- AB = b² - 1- BC = a²- CA = 2aSo, triangle inequalities would be:1. AB + BC > CA2. BC + CA > AB3. CA + AB > BCLet me write each inequality out with the given expressions.Starting with the first inequality: AB + BC > CAThat translates to (b² - 1) + a² > 2aSimplifying that: b² + a² - 1 > 2aSo, b² + a² - 2a - 1 > 0. Maybe rearrange terms: a² - 2a + b² - 1 > 0Hmm, not sure if that helps yet. Let's do the next inequality.Second inequality: BC + CA > ABWhich is a² + 2a > b² - 1Simplify: a² + 2a + 1 > b²Wait, that's a perfect square on the left. So, (a + 1)² > b²Taking square roots (since a and b are positive integers), this implies that a + 1 > bSo, a + 1 > b. Therefore, b < a + 1. Since both a and b are integers greater than 1, this means that b ≤ a. Because if b were equal to a + 1, the inequality would not hold. So, b must be less than or equal to a.Wait, hold on. Let me check that again. If (a + 1)² > b², then taking square roots gives a + 1 > |b|. But since b is positive, it's a + 1 > b. Therefore, b must be less than a + 1. Since a and b are integers, this translates to b ≤ a. So, b is at most a. So, b - a would be at most 0, but since both are greater than 1, maybe there's a specific case here. Wait, but the problem asks for b - a, so perhaps it's a negative number? But the answer might be positive if my reasoning is off. Let me hold off on that until I check the third inequality.Third inequality: CA + AB > BCWhich is 2a + (b² - 1) > a²Simplify: 2a + b² - 1 - a² > 0Rearranging terms: -a² + 2a + b² - 1 > 0Or, b² - a² + 2a - 1 > 0Hmm, maybe factor b² - a² as (b - a)(b + a). Let's see:(b - a)(b + a) + 2a - 1 > 0Not sure if that helps. Alternatively, let's write it as b² > a² - 2a + 1Wait, a² - 2a + 1 is (a - 1)². So, the inequality becomes b² > (a - 1)²Taking square roots again, since both sides are positive, this gives b > a - 1. Since a and b are integers greater than 1, this means that b ≥ a - 1 + 1 = a. So, b ≥ a.Wait, hold on. Let me check:If b² > (a - 1)², then taking square roots gives |b| > |a - 1|. Since a and b are positive integers greater than 1, a - 1 is at least 1 (since a ≥ 2), and b is at least 2. So, b > a - 1. Since they are integers, this implies that b ≥ (a - 1) + 1 = a. Therefore, b ≥ a.So from the second inequality, we have b ≤ a, and from the third inequality, we have b ≥ a. Therefore, combining both, we must have b = a.Wait, that seems to pin down b = a. So then, if b = a, then we can substitute into one of the inequalities to find possible values of a (and thus b). Let's see.So, since b = a, let's go back to the second inequality:(a + 1)² > b² ⇒ (a + 1)² > a² ⇒ a² + 2a + 1 > a² ⇒ 2a + 1 > 0, which is always true since a is at least 2. So that doesn't give us any new information.Let me check the first inequality again with b = a:First inequality: a² + a² - 1 > 2a ⇒ 2a² - 1 > 2a ⇒ 2a² - 2a - 1 > 0Let me solve 2a² - 2a - 1 > 0.Quadratic equation: 2a² - 2a - 1 = 0Discriminant: 4 + 8 = 12Solutions: [2 ± sqrt(12)] / 4 = [2 ± 2*sqrt(3)] / 4 = [1 ± sqrt(3)] / 2So, the roots are approximately (1 + 1.732)/2 ≈ 1.366 and (1 - 1.732)/2 ≈ -0.366Therefore, the inequality 2a² - 2a - 1 > 0 holds when a < (-0.366) or a > 1.366. Since a is an integer greater than 1, a ≥ 2. So, for a ≥ 2, this inequality holds. So no problem there.Now, let's check the third inequality with b = a:Third inequality: 2a + (a² - 1) > a² ⇒ 2a + a² - 1 > a² ⇒ 2a - 1 > 0 ⇒ 2a > 1 ⇒ a > 0.5, which is already satisfied since a is at least 2.So, all inequalities are satisfied as long as b = a and a ≥ 2. However, this seems like there's still multiple possible solutions. But wait, the problem says "Find b - a". If b = a, then b - a = 0. But the problem states that a and b are integers greater than 1. So, if the answer is zero, that might be possible. However, maybe there are more constraints?Wait, perhaps there's a unique solution when considering the actual lengths. Let me check the given side lengths again:AB = b² - 1, BC = a², CA = 2a.Since b = a, AB becomes a² - 1. So, the sides are:AB = a² - 1BC = a²CA = 2aSo, now, we have triangle sides: a² - 1, a², and 2a. Let's check if these can form a valid triangle.We already checked the triangle inequalities, which hold for a ≥ 2. But maybe there's a specific a where these lengths correspond to an actual triangle. But since the problem says "a, b are integers greater than 1", and given that a and b can be any integers as long as the inequalities hold, but since b = a, perhaps there is a unique solution. Wait, maybe I need to check for Pythagorean triples or something?Wait, but it's a general triangle, not necessarily right-angled. Hmm. Let me think.Alternatively, maybe there's another relationship here. Let's try plugging in small integer values for a starting from 2 and see if the sides make sense.Let's try a = 2 (so b = 2 as well):AB = 2² - 1 = 4 - 1 = 3BC = 2² = 4CA = 2*2 = 4So, sides 3, 4, 4. That is a valid triangle. Indeed, 3 + 4 > 4, 4 + 4 > 3, 3 + 4 > 4. All inequalities hold. So that's a valid triangle.Check if there are other possible a. Let's try a = 3:AB = 9 - 1 = 8BC = 9CA = 6Check triangle inequalities:8 + 9 > 6: 17 > 6, yes9 + 6 > 8: 15 > 8, yes6 + 8 > 9: 14 > 9, yesSo, 8, 9, 6 is a valid triangle.Similarly, a = 4:AB = 16 - 1 = 15BC = 16CA = 8Check inequalities:15 + 16 > 8: 31 > 8, yes16 + 8 > 15: 24 > 15, yes8 + 15 > 16: 23 > 16, yesSo, 15, 16, 8 is also valid.Wait, but the problem says "Find b - a". If in all these cases, b = a, then b - a = 0. But the problem might be expecting a different answer. Wait, maybe I made a mistake in the reasoning.Wait, let's go back. The problem states that a and b are integers greater than 1, and asks for b - a. If all cases where b = a satisfy the triangle conditions, then the answer could be zero, but I need to check if there's an additional constraint. Wait, maybe there's a unique solution where the triangle is possible only for specific a and b.Wait, perhaps there's a misinterpretation here. Wait, the problem says "Find b - a". If the answer is zero, then that's possible, but the problem might have a unique answer. Let me check again.Wait, when a = 2, b = 2, sides are 3, 4, 4.When a = 3, b = 3, sides are 8, 9, 6.But the problem says "Find b - a". So, unless there's a unique solution, but according to the given problem statement, it's possible that the answer is 0, but maybe not. Wait, perhaps there's a different approach here. Maybe the triangle is a right triangle? Let's check for a = 2.If a = 2, sides 3, 4, 4. Not a right triangle because 3² + 4² = 9 + 16 = 25 ≠ 4². Wait, 4² is 16, so that's not. Similarly, 3² + 4² ≠ 4². So not a right triangle.If a = 3, sides 8, 9, 6. Check if 6² + 8² = 36 + 64 = 100 = 10². 9² is 81. So, no, not a right triangle.Wait, perhaps there's another condition here. Maybe the triangle has integer sides and is Heronian (integer area). Let's check.For a = 2, sides 3, 4, 4. The area can be calculated using Heron's formula: semi-perimeter s = (3 + 4 + 4)/2 = 11/2 = 5.5. Area = sqrt(5.5*(5.5 - 3)*(5.5 - 4)*(5.5 - 4)) = sqrt(5.5*2.5*1.5*1.5). Hmm, 5.5*2.5 = 13.75, 1.5*1.5 = 2.25, so total is 13.75*2.25 = 30.9375. sqrt(30.9375) ≈ 5.56. Not an integer. So non-integer area.For a = 3, sides 6, 8, 9. Semi-perimeter s = (6 + 8 + 9)/2 = 23/2 = 11.5. Area = sqrt(11.5*(11.5 - 6)*(11.5 - 8)*(11.5 - 9)) = sqrt(11.5*5.5*3.5*2.5). This is a bit messy, but let's compute it: 11.5*5.5 = 63.25, 3.5*2.5 = 8.75, so 63.25*8.75 = 554.6875. sqrt(554.6875) ≈ 23.55. Not integer either.So, even though the areas aren't integers, the problem doesn't specify that the triangle needs to be Heronian, just that the sides are integers. So, multiple solutions exist where a = b. Therefore, the answer would be 0. But wait, maybe the problem expects a different answer. Let me check again the problem statement.Wait, the problem says "Find b - a". If the answer is 0, that's possible. But maybe there's a unique solution here. Wait, in the problem statement, maybe the triangle is determined uniquely by the given side lengths. Let me see.Wait, the sides are given as AB = b² - 1, BC = a², CA = 2a. So, if b = a, then AB = a² - 1, BC = a², CA = 2a. So, the sides depend on a. However, the problem doesn't mention any other conditions. So, unless there's a miscalculation here, the answer should be 0. But I need to verify again the steps.Wait, earlier, from the second inequality, we had b ≤ a, and from the third inequality, we had b ≥ a, leading to b = a. Therefore, according to the triangle inequalities, the only possibility is b = a. Therefore, b - a = 0. So, is that the answer? But let me check with another approach.Alternatively, maybe we can use the Law of Cosines here. Let's see. If we set up equations using the Law of Cosines, but since we don't know any angles, that might not be helpful. Alternatively, maybe the sides form a Pythagorean triple. Wait, but earlier examples didn't show that.Wait, let's try to see if with b = a + k, then see if k can be non-zero, but according to inequalities, k must be 0. So, that might not work.Wait, another thought: since the sides are AB = b² -1, BC = a², CA = 2a. Maybe there is a specific a and b that makes these sides correspond to a known triangle or satisfy another condition. But since the problem doesn't specify any other condition, like a right angle or area, the only constraints are the triangle inequalities. Which, as per the earlier reasoning, force b = a. Therefore, the answer is 0.Wait, but the problem is presented in a way that suggests a unique answer, and 0 is possible, but maybe there's a miscalculation here. Let me check again the critical step where from the second inequality we get b ≤ a, and from the third inequality b ≥ a, leading to b = a.Wait, the second inequality: (a + 1)² > b² => a + 1 > b. Therefore, b < a + 1. Since a and b are integers, this is equivalent to b ≤ a.Third inequality: b² > (a - 1)² => b > a - 1. Since they are integers, this gives b ≥ a.Therefore, combining b ≤ a and b ≥ a, we get b = a. So, this is correct.Therefore, the answer is 0. But let me check with a = 2, b = 2. Then sides are 3, 4, 4. Works. Similarly, a = 3, b = 3: 8, 9, 6. Also works. So, multiple solutions. But the problem says "Find b - a". If it's always 0, then the answer is 0. But maybe the problem expects a different answer? Wait, maybe I made a mistake in the inequality direction.Wait, let me check the third inequality again. Third inequality: CA + AB > BC => 2a + (b² - 1) > a² => 2a + b² - 1 > a² => b² > a² - 2a + 1 => b² > (a - 1)^2. Therefore, b > a - 1 or b < -(a - 1). Since b is positive, we can ignore the negative. So, b > a - 1. But since a and b are integers greater than 1, if a is 2, then a - 1 is 1, so b > 1. Which is already satisfied. If a is 3, then a - 1 is 2, so b > 2. Which is satisfied since b ≥ 3 (from b ≥ a). Wait, hold on, if a = 3, then from earlier, since b ≥ a, b ≥ 3, so that's okay.Wait, so the third inequality gives b > a - 1, which for integer b and a, translates to b ≥ a (since if a - 1 is not an integer, but since a is integer, a -1 is integer, so b must be at least (a - 1) + 1 = a). Therefore, b ≥ a.From the second inequality, (a + 1)^2 > b^2 => a + 1 > b, so b ≤ a. Therefore, combining, b = a.Therefore, this is the only possibility.Hence, the answer is b - a = 0.But the problem might have a trick here. Let me check if there's a case where b ≠ a but the inequalities still hold. Wait, for example, take a = 2, b = 3.But if a = 2, then CA = 4, BC = 4, AB = b² -1 = 9 -1 = 8. So, sides would be 8, 4, 4. Wait, 8, 4, 4: but 4 + 4 is not greater than 8. So, that's not a valid triangle. Hence, if b = 3, a = 2, triangle inequality fails.Similarly, if a = 3, b = 4: AB = 16 - 1 = 15, BC = 9, CA = 6. Then check triangle inequalities: 15 + 9 > 6 (yes), 9 + 6 > 15? 15 > 15? No, 15 is not greater than 15. So, that's invalid.Alternatively, if a = 4, b = 5: AB = 25 -1 =24, BC =16, CA=8. Check triangle inequalities: 24 +16 >8 (yes), 16 +8 >24? 24 >24? No, equal. So, invalid.Therefore, indeed, when b > a, the triangle inequality fails. Similarly, if b < a, then let's say a =3, b=2: AB=4 -1=3, BC=9, CA=6. Then sides are 3,9,6. Check inequalities: 3 + 9 >6 (yes), 9 +6 >3 (yes), 6 +3 >9? 9 >9? No, equality. So invalid.Therefore, only when b = a, the triangle inequalities hold. So, the answer must be 0. Therefore, I think the answer is 0.But the problem says "Find b - a". If the answer is 0, then that's the answer. But maybe the problem is from a source where 0 is not the expected answer. Wait, let me check again. Maybe I made a mistake in interpreting the triangle sides.Wait, the problem states:In triangle ABC, AB = b² - 1, BC = a², CA = 2a.So, AB is opposite to angle C, BC is opposite to angle A, and CA is opposite to angle B. Wait, no, in standard notation, AB is the side opposite angle C, BC is opposite angle A, and AC is opposite angle B. Wait, but the problem didn't specify which sides correspond to which. Wait, no, the problem just says triangle ABC with sides AB = b² -1, BC = a², CA = 2a. So, AB is between points A and B, BC is between B and C, CA is between C and A.But regardless of that, the triangle inequalities are based on the lengths. So, regardless of labels, the inequalities must hold.Wait, but maybe in the problem, there was a figure or specific orientation, but since there is no figure, my previous reasoning still applies. So, I think my conclusion that b - a = 0 is correct.But to be thorough, let's check with a = 2, b = 2:Sides AB = 3, BC =4, CA=4. So, triangle with sides 3,4,4. That's an isoceles triangle with two sides of 4 and base 3. Valid.Another check: a = 3, b =3: sides 8,9,6. That's a scalene triangle. Valid.Another check: a =4, b=4: sides 15,16,8. 15 +16 >8, 16+8>15, 15+8>16. 23>16. Yes, valid.So, multiple solutions, but in each case, b - a =0. Therefore, the answer is 0.Wait, but I'm a bit confused because the problem says "Find b - a", which is zero. But maybe the problem expects a positive integer answer. Wait, perhaps I made a mistake in the inequalities. Let me check again.Wait, the second inequality: BC + CA > AB => a² + 2a > b² -1 => a² + 2a +1 > b² => (a +1)^2 > b² => a +1 > b.Third inequality: CA + AB > BC => 2a + (b² -1) > a² => b² > a² - 2a +1 => b² > (a -1)^2 => b > a -1.Since a and b are integers greater than 1, combining these:From second inequality: b < a +1 => b ≤ a.From third inequality: b > a -1 => b ≥ a (since a -1 +1 =a). So, b ≥ a.Therefore, combining both: b =a.Therefore, the answer is 0. Hence, I think the answer is 0.But let me check again with a=2, b=2, sides 3,4,4: valid.But in the problem statement, maybe there's a different configuration. Wait, perhaps the problem assumes that the sides correspond to different sides. Wait, AB is opposite angle C, BC is opposite angle A, CA is opposite angle B. But even so, the triangle inequalities are about the lengths, not about the angles. So regardless, the conclusion remains the same.Alternatively, maybe the problem is in a right triangle? Let's check if for some a, the triangle is right-angled.For a=2, sides 3,4,4. Not a right triangle.For a=3, sides 8,9,6. Let's check: 6² +8²=36+64=100=10²≠9². So not a right triangle.For a=4, sides 15,16,8. 8² +15²=64+225=289=17²≠16². So, not a right triangle. But 8,15,17 is a Pythagorean triple. Wait, so 8,15,17 is a right triangle, but here sides are 8,15,16. So, not a right triangle.So, no, even if we tried, it's not a right triangle. Therefore, the answer must be 0.Alternatively, maybe I misapplied the triangle inequality. Let me check the steps again.From second inequality: a² + 2a > b² -1 => (a +1)^2 > b² => a +1 > b. So, since a and b are integers, a +1 > b => b ≤a.Third inequality: 2a + b² -1 > a² => b² > a² -2a +1 => b² > (a -1)^2 => b > a -1. Since a and b are integers, this implies b ≥a.Therefore, b must be equal to a. Hence, answer is 0.Therefore, I think the answer is boxed{0}.But wait, the problem is from an Olympiad or competition, usually answers are positive integers. Hmm. Maybe I made a mistake here. Let me check once again.Suppose a=2, b=2: sides 3,4,4. Valid.a=3, b=3: 6,9,8. Valid.a=4, b=4:8,16,15. Valid.But is there a possible case where b -a is not zero? For example, a=2, b=1. But b must be greater than 1. So, b=1 is invalid.Alternatively, a=3, b=2: sides AB=4-1=3, BC=9, CA=6. Then sides 3,9,6. Check inequalities: 3+6=9, which is not greater than 9. So, invalid.Thus, no. Hence, only possible when b=a. Therefore, answer is 0. So, boxed{0} is the answer.Final Answerboxed{0}</think>Given triangle (ABC) with sides (AB = b^2 - 1), (BC = a^2), and (CA = 2a), where (a) and (b) are integers greater than 1, we need to find (b - a).We use the triangle inequality theorem to set up the following inequalities:1. (AB + BC > CA)2. (BC + CA > AB)3. (CA + AB > BC)Substituting the given side lengths into these inequalities:1. ((b^2 - 1) + a^2 > 2a)2. (a^2 + 2a > b^2 - 1)3. (2a + (b^2 - 1) > a^2)For the second inequality:[a^2 + 2a > b^2 - 1 implies a^2 + 2a + 1 > b^2 implies (a + 1)^2 > b^2 implies a + 1 > b]Since (a) and (b) are integers, this implies (b leq a).For the third inequality:[2a + b^2 - 1 > a^2 implies b^2 > a^2 - 2a + 1 implies b^2 > (a - 1)^2 implies b > a - 1]Since (a) and (b) are integers, this implies (b geq a).Combining the results from the second and third inequalities, we get:[b leq a quad text{and} quad b geq a implies b = a]Thus, (b - a = 0).The final answer is (boxed{0}).,<think>Okay, let's see. I need to find the value of b - a in triangle ABC where the sides are given as AB = b² - 1, BC = a², and CA = 2a. Both a and b are integers greater than 1. Hmm, triangles, integer sides, okay.First, I remember that for any triangle, the sum of any two sides must be greater than the third side. This is called the triangle inequality. So, I need to apply this rule to all three combinations of sides. Let me write down the inequalities.So, the sides are AB = b² - 1, BC = a², and CA = 2a. Let's denote them as follows for clarity:AB = b² - 1BC = a²CA = 2aSo, the triangle inequalities would be:1. AB + BC > CA2. BC + CA > AB3. CA + AB > BCLet me substitute the expressions into each inequality.First inequality: AB + BC > CAThat is, (b² - 1) + a² > 2aSimplify: b² + a² - 1 > 2aSecond inequality: BC + CA > ABThat is, a² + 2a > b² - 1Simplify: a² + 2a + 1 > b²Wait, that can be written as (a + 1)² > b² because a² + 2a + 1 is (a + 1)². So, (a + 1)² > b², which implies that a + 1 > b, since both a and b are positive integers. Therefore, b must be less than a + 1. So, b ≤ a. Hmm, interesting. So that gives us a relationship between b and a.Third inequality: CA + AB > BCThat is, 2a + (b² - 1) > a²Simplify: 2a + b² - 1 > a²Let me rearrange this: b² > a² - 2a + 1Which is b² > (a - 1)²Since both sides are squares of integers, this implies that b > a - 1. Since b and a are integers greater than 1, this tells us that b is at least a - 1 + 1 = a. Wait, but from the second inequality we had that b ≤ a. So combining these two results: b > a - 1 and b ≤ a. Since b must be an integer, this implies that b can be either a or a - 1. But b and a are integers greater than 1.Wait, let's clarify. From the second inequality, we have (a + 1)² > b², so a + 1 > b. Therefore, b < a + 1. Since both are integers, this implies that b ≤ a. From the third inequality, we have b² > (a - 1)², which implies that b > a - 1. Since a and b are integers, this implies that b ≥ a (since if b > a - 1, and b is an integer, then if a - 1 is not an integer, but wait, a is an integer, so a - 1 is an integer. So b has to be greater than a - 1, so the smallest integer greater than a - 1 is a. So, b ≥ a. Therefore, combining both inequalities: from second inequality, b ≤ a, and from third inequality, b ≥ a. Therefore, the only possibility is that b = a.Wait, is that possible? If b = a, then let's check the first inequality. Let's see:First inequality: b² + a² - 1 > 2aIf b = a, then substituting:a² + a² - 1 > 2a → 2a² - 1 > 2a → 2a² - 2a - 1 > 0Let me solve 2a² - 2a - 1 > 0.Quadratic equation: 2a² - 2a - 1 = 0Discriminant: ( -2 )² - 4*2*(-1) = 4 + 8 = 12Solutions: [2 ± sqrt(12)]/(2*2) = [2 ± 2*sqrt(3)]/4 = [1 ± sqrt(3)]/2Approximately, sqrt(3) ≈ 1.732, so positive root: (1 + 1.732)/2 ≈ 1.366Negative root is less than 0. So the inequality 2a² - 2a - 1 > 0 holds when a > 1.366 or a < -0.366. Since a is an integer greater than 1, a ≥ 2. Therefore, for a ≥ 2, this inequality is satisfied. So, first inequality holds for a ≥ 2 if b = a.But wait, let's check with actual values. Let's suppose a = 2, then b = a = 2.Check all three inequalities:First inequality: AB + BC > CAAB = b² - 1 = 4 - 1 = 3BC = a² = 4CA = 2a = 4So 3 + 4 = 7 > 4. True.Second inequality: BC + CA > AB4 + 4 = 8 > 3. True.Third inequality: CA + AB > BC4 + 3 = 7 > 4. True.So, triangle with sides 3, 4, 4 is valid. So, a = 2, b = 2, so b - a = 0. But the problem states that a and b are integers greater than 1. So 0 is a possible answer? Wait, but let's check the problem again. The problem says "a, b are integers greater than 1". So a and b are at least 2. So if a = 2, b = 2, that's allowed. Then b - a = 0. Hmm.But let's check if there are other possibilities. Wait, earlier reasoning concluded that b must be equal to a, but let me verify that.From the second inequality, we had (a + 1)² > b², so a + 1 > b.From the third inequality, we had b² > (a - 1)², so b > a - 1.But since a and b are integers, so:From a + 1 > b ⇒ b ≤ aFrom b > a - 1 ⇒ b ≥ a (since if a - 1 is, say, 2 - 1 = 1, then b > 1, but since b is integer greater than 1, so b ≥ 2. Wait, no. Wait, if a is 3, then a - 1 = 2, so b > 2, so b ≥ 3. Wait, but if a is 3, then from the first part, b ≤ 3.Wait, perhaps my earlier conclusion that b must equal a is incorrect. Let me re-examine.Suppose a is 2.From the third inequality: b² > (2 - 1)² ⇒ b² > 1 ⇒ b > 1. Since b is integer greater than 1, so b ≥ 2.From the second inequality: (2 + 1)² > b² ⇒ 9 > b² ⇒ b < 3. Since b is integer, so b ≤ 2.Therefore, b must be 2. Hence, b = a.Similarly, if a = 3.Third inequality: b² > (3 - 1)² ⇒ b² > 4 ⇒ b > 2 ⇒ b ≥ 3.Second inequality: (3 + 1)² > b² ⇒ 16 > b² ⇒ b < 4 ⇒ b ≤ 3.Thus, b = 3. So again, b = a.Wait, so for any a ≥ 2, b must equal a. Therefore, in all cases, b = a. So, b - a = 0.But let's test with a = 3. Then, sides would be AB = 9 - 1 = 8, BC = 9, CA = 6.Check triangle inequalities:8 + 9 > 6 ⇒ 17 > 6. True.9 + 6 > 8 ⇒ 15 > 8. True.6 + 8 > 9 ⇒ 14 > 9. True. So triangle with sides 8, 9, 6 is valid. So yes, a = 3, b = 3, so b - a = 0.But the problem says "Find b - a". If the answer is 0, then why is the problem structured this way? Maybe I made a mistake here. Wait, maybe there's another possibility where b ≠ a? Let me check.Wait, suppose that in the third inequality, b² > (a - 1)². So, it's possible that b could be equal to a, but if a - 1 is not an integer? Wait, no, a is an integer, so a - 1 is integer. So, the inequality b² > (a - 1)² implies that |b| > |a - 1|. Since both are positive integers, this means b > a - 1. Therefore, b can be a - 1 + 1 = a, or higher. But combined with the second inequality (a + 1)² > b², which gives b < a + 1, so b ≤ a. Therefore, b must be between a and a. So, only possible if b = a.Therefore, in all cases, b must equal a. Therefore, b - a = 0.But let me check with a = 4.AB = 16 - 1 = 15, BC = 16, CA = 8.Check inequalities:15 + 16 > 8 → 31 > 8. True.16 + 8 > 15 → 24 > 15. True.8 + 15 > 16 → 23 > 16. True. So, valid triangle.Therefore, seems like for any a ≥ 2, b = a gives a valid triangle. Hence, the answer is 0.But the problem says "Find b - a", and since the problem is from an Olympiad or competition, perhaps expecting a different answer. Maybe my reasoning is missing something.Wait, let's check if there are other possibilities where b ≠ a. Let's see. For example, suppose a = 2, then from second inequality, b < 3, so b = 2. From third inequality, b > 1, so b = 2. So only possibility.If a = 3, then second inequality gives b < 4, so b = 3. Third inequality gives b > 2, so b = 3. Similarly, for a = 4, b = 4. So, seems like b must equal a. Therefore, answer is 0.But maybe I made a mistake in interpreting the inequalities. Let me check again.First inequality: (b² - 1) + a² > 2a → b² + a² - 1 > 2a.Second inequality: a² + 2a > b² - 1 → a² + 2a + 1 > b² → (a + 1)^2 > b² → a + 1 > b.Third inequality: 2a + b² - 1 > a² → b² > a² - 2a + 1 → b² > (a - 1)^2 → b > a - 1.So, combining the second and third inequalities: a - 1 < b < a + 1. Since a and b are integers, this implies b is between (a - 1 + 1) and (a + 1 - 1). Wait, no. Wait, the inequalities are a - 1 < b < a + 1. So, since a and b are integers, this implies that b can be equal to a or a. Because between a -1 and a +1, the integer values are a -1, a, a +1. But since b must be greater than a -1 and less than a +1, and since b is integer, the possible values are a. Because if a -1 < b < a +1, then b must be a. For example, if a is 2, then b must be between 1 and 3, but since b is greater than 1, it can be 2 or 3. Wait, wait, no. Wait, let's take specific numbers.If a = 2:From second inequality: b < 3 (since a +1 =3). From third inequality: b >1 (since a -1 =1). Therefore, b can be 2. Since b must be integer greater than 1. So, b=2.If a=3:From second inequality: b <4. From third inequality: b>2. So, b=3.If a=4:b <5 and b>3. So, b=4.Therefore, in all cases, b=a. Therefore, the difference b -a=0.But the problem is presented in a way that expects a non-zero answer. Maybe I made a mistake here.Wait, let me check again with a=2, b=2:AB = 4 -1 =3, BC=4, CA=4. So triangle sides 3,4,4. That's a valid triangle. Similarly, with a=3, sides 8,9,6. Also valid. So, perhaps the answer is indeed 0. Maybe the problem is designed to test the triangle inequalities and how they constrain b to equal a, leading to a difference of 0.Alternatively, maybe I need to check the first inequality again. For a=2, b=2:First inequality: 3 + 4 >4 →7>4: True.But what if there is a case where b can be different? Wait, suppose a=2 and b=3. Then check the inequalities.But if a=2, then second inequality: (2 +1)^2 >b² →9> b². So, b can be 2 or 1. But b must be greater than1, so b=2. So b=3 is not allowed here.Wait, if someone tries to take a=2, b=3:AB=9 -1=8, BC=4, CA=4.Check triangle inequalities:8 +4 >4? 12>4: True.4 +4 >8? 8>8: No, 8 is not greater than8. So inequality fails. Hence, invalid triangle. Hence, b=3 is invalid here.Similarly, if a=3, trying b=4:AB=16 -1=15, BC=9, CA=6.Check inequalities:15 +9 >6: 24>6: True.9 +6 >15: 15>15: No, equality holds. Not valid.So, that's invalid. Hence, the only possibility is b=a.Therefore, the answer is 0. So, I think the answer is boxed{0}.But just to be thorough, let me check another value. Let's take a=5, then b must be 5.AB=25 -1=24, BC=25, CA=10.Check inequalities:24 +25 >10: 49>10: True.25 +10 >24: 35>24: True.10 +24 >25: 34>25: True. Valid triangle.Hence, works. So, unless there's a case where b can be different, but from the inequalities, seems impossible. Hence, answer is 0.Final Answerboxed{0}</think>To solve the problem, we need to find the value of ( b - a ) in triangle ( ABC ) where the sides are given as ( AB = b^2 - 1 ), ( BC = a^2 ), and ( CA = 2a ), with ( a ) and ( b ) being integers greater than 1. We start by applying the triangle inequality conditions:1. ( AB + BC > CA )2. ( BC + CA > AB )3. ( CA + AB > BC )Substituting the given side lengths into these inequalities:1. ( (b^2 - 1) + a^2 > 2a )2. ( a^2 + 2a > b^2 - 1 )3. ( 2a + (b^2 - 1) > a^2 )Analyzing the second inequality:[ a^2 + 2a + 1 > b^2 ]This can be rewritten as:[ (a + 1)^2 > b^2 ]which implies:[ a + 1 > b ]Analyzing the third inequality:[ 2a + b^2 - 1 > a^2 ]This can be rewritten as:[ b^2 > (a - 1)^2 ]which implies:[ b > a - 1 )Combining the results from the second and third inequalities:[ a - 1 < b < a + 1 ]Since ( a ) and ( b ) are integers, this implies:[ b = a ]We verify this result by substituting ( b = a ) into the first inequality:[ (a^2 - 1) + a^2 > 2a ][ 2a^2 - 1 > 2a ][ 2a^2 - 2a - 1 > 0 ]This quadratic inequality holds for ( a geq 2 ), which is satisfied since ( a ) is an integer greater than 1. Checking specific values of ( a ) (e.g., ( a = 2, 3, 4 )) confirms that the triangle inequalities are satisfied with ( b = a ).Thus, the value of ( b - a ) is:[ boxed{0} ]]
🔑:Since in a triangle, the sum of any two sides must be greater than the third side, we have:BC + AC > ABSubstituting the given values, we get:a^2 + 2a > b^2 - 1Rearranging and adding 1 to both sides, we obtain:a^2 + 2a + 1 > b^2This simplifies to:(a + 1)^2 > b^2Since a and b are integers greater than 1, it follows that:a + 1 > bTherefore, we have:a geq bSimilarly, since the difference between any two sides of a triangle must be less than the third side, we have:BC - AC < ABSubstituting the given values, we get:a^2 - 2a < b^2 - 1Rearranging and adding 1 to both sides, we obtain:a^2 - 2a + 1 < b^2This simplifies to:(a - 1)^2 < b^2Since a and b are integers greater than 1, it follows that:a - 1 < bTherefore, we have:a leq bCombining the two results, we conclude that:a = bTherefore, the difference b - a is:boxed{0}This problem primarily examines the application of the triangle inequality theorem, which states that the sum of the lengths of any two sides of a triangle must be greater than the length of the remaining side, and the difference between the lengths of any two sides of a triangle must be less than the length of the remaining side. The problem is comprehensive and not very difficult.
❓:If m and n satisfy |m-2|+left(n-2023right)^{2}=0, then m^{-2}+n^{0}=______.
🧠:[<think>Alright, so I need to solve this problem where m and n satisfy the equation |m - 2| + (n - 2023)² = 0, and then find the value of m⁻² + n⁰. Hmm, okay. Let me start by understanding what this equation means.First, I know that absolute value expressions, like |m - 2|, are always non-negative. Similarly, any squared term, such as (n - 2023)², is also non-negative. So, if I add two non-negative numbers together and the sum is zero, each of them must individually be zero. Because the only way two non-negative numbers add up to zero is if both are zero. Otherwise, their sum would be at least one of them being positive, making the total positive.So, that means |m - 2| has to be zero and (n - 2023)² has to be zero. Let me write that down:1. |m - 2| = 02. (n - 2023)² = 0Solving each equation separately. Starting with the first one: |m - 2| = 0. The absolute value of a number is zero only when the number inside is zero. So, m - 2 = 0. Solving for m, add 2 to both sides: m = 2. Got that.Next equation: (n - 2023)² = 0. A square of a real number is zero only when the number itself is zero. So, n - 2023 = 0. Solving for n, add 2023 to both sides: n = 2023. Okay, so m is 2 and n is 2023. Let me confirm that these values satisfy the original equation. Plugging into |m - 2| + (n - 2023)²:|2 - 2| + (2023 - 2023)² = 0 + 0 = 0. Yep, that works. So the values of m and n are indeed 2 and 2023 respectively.Now, the problem asks for m⁻² + n⁰. Let me parse that. m⁻² is the same as 1 over m squared, and n⁰ is any non-zero number to the power of zero, which is 1. So, n⁰ should be 1 regardless of n (as long as n isn't zero, but n is 2023 here, which is definitely not zero). So, n⁰ = 1. Then, m⁻² is 1/(m²). Since m is 2, m² is 4, so 1/4. Therefore, m⁻² + n⁰ = 1/4 + 1.Wait, adding 1/4 and 1. Let me compute that. 1 is the same as 4/4, so 1/4 + 4/4 = 5/4. So, 5 over 4. Which is 1.25 in decimal. But the answer should be in a fraction, probably, since the question is mathematical. So, 5/4.Let me double-check my steps to make sure I didn't make a mistake. Starting with the original equation: sum of two non-negatives equals zero, so both must be zero. That gives m = 2, n = 2023. Then compute m⁻² + n⁰. m⁻² is 1/(2)² = 1/4. n⁰ is 1. So 1/4 + 1 = 5/4. Hmm. That seems straightforward.Wait a second, is there any trick here that I might have missed? Like, maybe considering other solutions for m and n? But no, absolute value and square are both non-negative, so the only solution is when both are zero. Therefore, m = 2 and n = 2023 are the only possible solutions. So the answer should indeed be 5/4. Let me write that in a box as per the instructions.Final AnswerThe value of (m^{-2} + n^{0}) is boxed{dfrac{5}{4}}.</think>Given the equation ( |m - 2| + (n - 2023)^2 = 0 ), we know that both the absolute value and the squared term must be non-negative. Therefore, each term must individually be zero for their sum to be zero. 1. Solving ( |m - 2| = 0 ): [ m - 2 = 0 implies m = 2 ]2. Solving ( (n - 2023)^2 = 0 ): [ n - 2023 = 0 implies n = 2023 ]Next, we need to find ( m^{-2} + n^0 ):- ( m^{-2} = frac{1}{m^2} = frac{1}{2^2} = frac{1}{4} )- ( n^0 = 1 ) (since any non-zero number to the power of zero is 1)Adding these results:[frac{1}{4} + 1 = frac{1}{4} + frac{4}{4} = frac{5}{4}]Thus, the value of ( m^{-2} + n^0 ) is (boxed{dfrac{5}{4}}).,<think>Okay, let me try to figure out this problem. So, the question is: If m and n satisfy |m - 2| + (n - 2023)² = 0, then what is m⁻² + n⁰? Hmm, let's break this down step by step.First, I remember that absolute value expressions like |m - 2| are always non-negative because absolute values can't be negative. Similarly, any squared term, like (n - 2023)², is also non-negative. So, we have the sum of two non-negative things equaling zero. The only way that can happen is if each of them is zero individually. Because if one was positive and the other was zero, their sum would be positive, not zero. So, both |m - 2| and (n - 2023)² must each equal zero.Let me write that out. If |m - 2| + (n - 2023)² = 0, then:1. |m - 2| = 02. (n - 2023)² = 0Solving the first equation: |m - 2| = 0. The absolute value of something is zero only if the inside is zero. So, m - 2 = 0, which means m = 2. That seems straightforward.Now the second equation: (n - 2023)² = 0. Again, a square is zero only if the inside is zero. Therefore, n - 2023 = 0, which implies n = 2023. Got that.So now we have m = 2 and n = 2023. The question asks for m⁻² + n⁰. Let me compute each part step by step.First, m⁻². Since m = 2, this is 2⁻². Remembering that a negative exponent means the reciprocal. So, 2⁻² = 1/(2²) = 1/4. Got that.Next, n⁰. Any non-zero number raised to the power of 0 is 1. Since n = 2023, which is definitely not zero, n⁰ = 2023⁰ = 1. So, that part is 1.Now, adding those two results together: 1/4 + 1. To add these, I can convert 1 to 4/4 to have a common denominator. So, 1/4 + 4/4 = 5/4. That simplifies to 1.25 in decimal, but since the question probably expects a fractional answer, 5/4 is the way to go.Let me just double-check to make sure I didn't make a mistake. Starting with the original equation: sum of two non-negatives equals zero, so each must be zero. Solving for m and n gives 2 and 2023. Then plugging into m⁻² + n⁰: 1/4 + 1. Yep, that's 5/4. Hmm, seems right.Wait, let me confirm the exponent rules again. m⁻² is definitely 1/m². So, 2⁻² is 1/(2²) = 1/4. Correct. And n⁰, anything (except maybe zero, but n is 2023 here) to the power of zero is 1. So that's correct too. Adding 1/4 + 1 gives 5/4. So, yeah, I think that's the right answer.Final Answerboxed{dfrac{5}{4}}</think>Given the equation ( |m - 2| + (n - 2023)^2 = 0 ), we know that both the absolute value and the squared term must each be zero because they are non-negative and their sum is zero.1. Solving ( |m - 2| = 0 ): [ m - 2 = 0 implies m = 2 ]2. Solving ( (n - 2023)^2 = 0 ): [ n - 2023 = 0 implies n = 2023 ]Next, we calculate ( m^{-2} + n^0 ):- ( m^{-2} = 2^{-2} = frac{1}{2^2} = frac{1}{4} )- ( n^0 = 2023^0 = 1 )Adding these results together:[frac{1}{4} + 1 = frac{1}{4} + frac{4}{4} = frac{5}{4}]Thus, the final answer is:[boxed{dfrac{5}{4}}]]
🔑:Given the equation |m-2|+left(n-2023right)^{2}=0, we can analyze it step by step.First, since the sum of an absolute value and a square is equal to zero, both terms must individually be equal to zero because both are always non-negative. This leads us to two separate equations:1. |m-2|=02. left(n-2023right)^{2}=0Solving the first equation for m gives us:[|m-2|=0 implies m-2=0 implies m=2]Solving the second equation for n gives us:[left(n-2023right)^{2}=0 implies n-2023=0 implies n=2023]Now, we substitute m=2 and n=2023 into the expression m^{-2}+n^{0}:[m^{-2}+n^{0}=2^{-2}+2023^{0}]Since any non-zero number raised to the power of 0 is 1, and 2^{-2} equals frac{1}{4}, we have:[2^{-2}+1=frac{1}{4}+1=frac{1}{4}+frac{4}{4}=frac{5}{4}]Therefore, the final answer is boxed{frac{5}{4}}.
❓:13. Let x_{1}, x_{2}, x_{3} be the roots of the equation x^{3}-17 x-18=0, with -4<x_{1}<-3, and 4<x_{3}<5.(1) Find the integer part of x_{2};(2) Find the value of arctan x_{1}+arctan x_{2}+arctan x_{3}.
🧠:[<think>Okay, so I need to solve this problem where we have a cubic equation x³ - 17x - 18 = 0, with roots x₁, x₂, x₃. The given information is that x₁ is between -4 and -3, and x₃ is between 4 and 5. The questions are: (1) Find the integer part of x₂; and (2) Find the value of arctan x₁ + arctan x₂ + arctan x₃. Hmm, let's take this step by step.First, part (1): Finding the integer part of x₂. So, we know the cubic equation has three real roots since the problem specifies intervals for two of them, and presumably, the third root is somewhere else. The cubic equation is x³ - 17x - 18 = 0. Let me recall that for cubic equations, the sum of the roots, product, etc., can be found using Vieta's formulas. Maybe that will help here.Vieta's formulas for a cubic equation ax³ + bx² + cx + d = 0 tell us that:x₁ + x₂ + x₃ = -b/ax₁x₂ + x₁x₃ + x₂x₃ = c/ax₁x₂x₃ = -d/aIn this equation, the cubic is x³ - 17x - 18 = 0, so coefficients are a=1, b=0 (since there's no x² term), c=-17, d=-18.Therefore, applying Vieta's formulas:Sum of roots: x₁ + x₂ + x₃ = -b/a = 0Sum of products two at a time: x₁x₂ + x₁x₃ + x₂x₃ = c/a = -17Product of roots: x₁x₂x₃ = -d/a = 18So, sum of roots is zero. That's useful. So, x₁ + x₂ + x₃ = 0. Therefore, x₂ = -x₁ -x₃.Given that x₁ is between -4 and -3, and x₃ is between 4 and 5. So, x₁ is, say, approximately -3.5, and x₃ is approximately 4.5. Then x₂ would be approximately -(-3.5) -4.5 = 3.5 -4.5 = -1. So, x₂ is around -1. So, the integer part of x₂ would be -1? But we need to be more precise.Wait, but if x₁ is between -4 and -3, and x₃ is between 4 and 5, then x₂ = -x₁ -x₃. Let's compute the possible ranges. The minimum x₂ can be is when x₁ is as large as possible (closest to -3) and x₃ is as large as possible (closest to 5). So x₂ = -(-3) -5 = 3 -5 = -2. The maximum x₂ can be is when x₁ is as small as possible (closest to -4) and x₃ is as small as possible (closest to 4). So x₂ = -(-4) -4 = 4 -4 = 0. Therefore, x₂ is between -2 and 0. So the integer part would be either -2, -1, or 0? Wait, but according to the problem, x₂ is a root. So we need to find where exactly x₂ is.Alternatively, maybe we can use the Intermediate Value Theorem. Since it's a cubic, it's continuous. Let's check the function f(x) = x³ -17x -18. We know the roots are x₁, x₂, x₃. We already have intervals for x₁ and x₃. Let's check the values around x between -2 and 0 to see where x₂ might be.First, check f(-2): (-2)³ -17*(-2) -18 = -8 +34 -18 = 8. So f(-2) = 8.f(-1): (-1)³ -17*(-1) -18 = -1 +17 -18 = -2. So f(-1) = -2.f(0): 0 -0 -18 = -18. So f(0) = -18.So between x=-2 and x=-1: f(-2)=8, f(-1)=-2. So by Intermediate Value Theorem, there is a root between -2 and -1. Similarly, between x=-1 and x=0: f(-1)=-2, f(0)=-18. So function goes from -2 to -18, which is decreasing. So no root there. Wait, but we already have three roots: x₁ between -4 and -3, x₂ somewhere, and x₃ between 4 and5.Wait, but the function at x=-4: f(-4)= (-4)^3 -17*(-4) -18 = -64 +68 -18 = (-64 +68)=4; 4 -18 = -14. So f(-4) = -14.At x=-3: f(-3)= (-27) -17*(-3) -18 = -27 +51 -18 = 6. So f(-3)=6. So the root x₁ is between -4 and -3 because the function crosses from -14 to 6.Similarly, x₃ is between 4 and5. Let's check f(4)=64 -68 -18= -22. f(5)=125 -85 -18=22. So crosses from -22 to22, so root between 4 and5.Now, for x₂: the third root. The sum of the roots is zero, so x₂ = -x₁ -x₃. Since x₁ is between -4 and -3, and x₃ is between4 and5, then x₂ is between -( (-4) +4 )=0 and -( (-3)+5 )=-2. Wait, that's conflicting with previous calculation. Wait: x₂ = -x₁ -x₃. If x₁ is in (-4, -3), then -x₁ is in (3,4). x₃ is in (4,5). So -x₁ -x₃ is in (3 -5, 4 -4)= (-2,0). So x₂ is between -2 and 0. So possible interval is from -2 to 0. But from the function f(x) evaluated at x=-2: f(-2)=8, x=-1: f(-1)=-2, x=0: -18. So between x=-2 and x=-1, the function crosses from 8 to -2, so there's a root there. That must be x₂. Then between x=-1 and x=0, function is decreasing from -2 to -18, so no root there. Therefore, x₂ must be between -2 and -1. Therefore, the integer part of x₂ is -2? Wait, but if x₂ is between -2 and -1, then the integer part is -2, since the integer part is the greatest integer less than or equal to x₂. For example, if x₂ is -1.5, the integer part is -2. So yes, the integer part is -2. Wait, but let's confirm this.Wait, but when I first approximated x₂ as around -1, but actually, the exact location is between -2 and -1. So the integer part is -2. Let's verify.Wait, but hold on. The problem states that x₁ is between -4 and -3, x₃ is between4 and5. The sum x₁ +x₂ +x₃=0, so x₂= -x₁ -x₃. Let's compute the range:x₁ is between -4 and -3, so -x₁ is between3 and4.x₃ is between4 and5, so -x₃ is between-5 and -4.Therefore, x₂= -x₁ -x₃ = (3 to4) + (-5 to -4) = (3 -5) to (4 -4) = (-2 to0). So x₂ is between-2 and0. But based on the function evaluations:f(-2)=8, f(-1)=-2, f(0)=-18. So between x=-2 and x=-1, function goes from 8 to -2, so crosses zero somewhere there. Hence, x₂ is between-2 and-1. Then between x=-1 and x=0, the function continues to decrease from -2 to -18, so no root there. Therefore, x₂ is indeed in (-2, -1). So the integer part of x₂ is -2. So answer to part (1) is -2? Wait, but the integer part is the floor function, right? So if x is between -2 and -1, the integer part is -2, because it's the greatest integer less than or equal to x. For example, -1.5's integer part is -2. So yes, the integer part is -2. Therefore, (1) is -2.Now, part (2): Find the value of arctan x₁ + arctan x₂ + arctan x₃. Hmm, need to compute the sum of arctans of the roots. Maybe there's a trigonometric identity that can help here, especially since the roots are related through the cubic equation. Alternatively, perhaps the sum of arctans can be related to some angle.Alternatively, consider the formula for tan(A + B + C). If we can find tan(arctan x₁ + arctan x₂ + arctan x₃), maybe that simplifies to something, and then take arctan of that. But it might be complicated. Alternatively, maybe the sum is a multiple of π or something like that. Let's try.Let me recall that arctan a + arctan b = arctan((a + b)/(1 - ab)) + kπ, where k is an integer depending on the quadrant. But when adding three terms, it's more complicated. Let's see.Let’s denote S = arctan x₁ + arctan x₂ + arctan x₃. We need to compute S. Let's compute tan S.Using the formula for tan(A + B + C):tan(A + B + C) = (tan A + tan B + tan C - tan A tan B tan C) / (1 - tan A tan B - tan A tan C - tan B tan C)In this case, tan A = x₁, tan B = x₂, tan C = x₃. So,tan S = (x₁ + x₂ + x₃ - x₁x₂x₃) / (1 - x₁x₂ - x₁x₃ - x₂x₃)But from Vieta's formulas, we know:x₁ + x₂ + x₃ = 0x₁x₂ + x₁x₃ + x₂x₃ = -17x₁x₂x₃ = 18Therefore, substituting these into the expression for tan S:tan S = (0 - 18) / (1 - (-17)) = (-18) / (1 +17) = (-18)/18 = -1Therefore, tan S = -1. So S is an angle whose tangent is -1. The arctangent function usually gives values between -π/2 and π/2, but since we are adding three arctans, the sum could be in a different interval.But tan S = -1 implies that S = arctan(-1) + kπ, where k is an integer. arctan(-1) is -π/4. However, the actual value of S depends on the individual arctans.Let's consider the individual values:x₁ is between -4 and -3, so arctan x₁ is between arctan(-4) and arctan(-3). arctan(-4) is approximately -1.3258 radians, and arctan(-3) is approximately -1.2490 radians. So arctan x₁ is between approximately -1.3258 and -1.2490, which is in the fourth quadrant (if we consider the principal value which is between -π/2 and π/2).x₂ is between -2 and -1, so arctan x₂ is between arctan(-2) ≈ -1.1071 and arctan(-1) = -π/4 ≈ -0.7854 radians.x₃ is between4 and5, so arctan x₃ is between arctan(4) ≈1.3258 and arctan(5)≈1.3734 radians.So summing them up:The sum S would be approximately (-1.3258) + (-1.1071) +1.3258 ≈ -1.1071, but that's just a rough estimate. Alternatively, maybe there's a cancellation. Wait, but arctan x₁ is negative, arctan x₂ is negative, arctan x₃ is positive. So the total sum would be a negative plus a negative plus a positive. Depending on the exact values, the sum could be negative or positive.But since tan S = -1, which we found earlier. So tan S = -1, which occurs at angles of -π/4, 3π/4, 7π/4, etc. So which one is it?To determine the correct value, we need to consider the approximate sum. Let's approximate each arctan:Let's take x₁ ≈ -3.5 (midpoint of -4 and -3). arctan(-3.5) ≈ ?Using a calculator, arctan(-3.5) ≈ -1.2925 radians.x₂ ≈ -1.5 (midpoint of -2 and -1). arctan(-1.5) ≈ -0.9828 radians.x₃ ≈4.5 (midpoint of 4 and5). arctan(4.5)≈1.3526 radians.Sum≈-1.2925 -0.9828 +1.3526≈ (-2.2753) +1.3526≈-0.9227 radians.But tan(-0.9227)≈tan(-π/4 -0.4636)≈? Let's see, tan(-0.9227)≈tan(-0.9227 + π)≈tan(2.2189)≈-1. So that's consistent with tan S = -1. But the actual sum is approximately -0.9227 radians, which is approximately -53 degrees, but arctan(-1) is -π/4≈-0.7854. Wait, but our approximate sum is -0.9227, which is less than -π/4. However, -0.9227 is equal to approximately -π/4 -0.1373. So how does that relate to the identity?But we know that tan S = -1, so S could be -π/4, 3π/4, -5π/4, etc. But depending on the actual value. However, our approximate sum is around -0.9227, which is more negative than -π/4≈-0.7854. So maybe S = -3π/4? Because -3π/4≈-2.356, which is more negative. Wait, but our approximate sum is only -0.9227. Wait, this seems conflicting. Wait, no. Wait, -0.9227 radians is approximately -53 degrees, but -3π/4 is -135 degrees. That's a big difference.Wait, perhaps my approximation is wrong. Let's check again.Wait, if x₁ is -3.5, arctan(-3.5)≈-1.2925 radians (which is about -74 degrees). x₂ is -1.5, arctan(-1.5)≈-0.9828 radians (≈-56 degrees). x₃ is4.5, arctan(4.5)≈1.3526 radians (≈77 degrees). Adding them: -74 -56 +77≈-53 degrees≈-0.925 radians. So approximately -0.925 radians, which is -53 degrees. However, tan(-53 degrees)≈-1.333, not -1. But earlier, we had tan S = -1. So there's a discrepancy here. So my approximation might be leading me astray.Wait, but the problem is exact. Maybe the sum is exactly -π/4, but our approximate calculation suggests otherwise. However, according to the earlier formula, tan S = -1, so S must be an angle where tangent is -1. The principal value is -π/4, but depending on the actual sum, it could be in another quadrant. So let's think.If the sum S is equal to arctan x₁ + arctan x₂ + arctan x₃, and we found that tan S = -1, then S is congruent to -π/4 modulo π. So S = -π/4 + kπ. To find k, we can approximate the sum.As per our earlier approximation, S≈-0.925 radians. -π/4≈-0.785, so -0.925 is less than -π/4. If we add π, we get -0.925 + π≈2.216 radians≈127 degrees. But 127 degrees is more than π/2, which might not make sense. Alternatively, maybe it's in the third quadrant. Wait, but individual arctans are:arctan x₁≈-1.2925 (Q4), arctan x₂≈-0.9828 (Q4), arctan x₃≈1.3526 (Q1). So sum is roughly (-1.2925 -0.9828) +1.3526≈(-2.2753) +1.3526≈-0.9227. So the sum is negative, around -0.9227, which is between -π/2 (-1.5708) and 0. So it's in the fourth quadrant. However, tan(-0.9227)=tan(-0.9227)=tan(-π/4 -0.1373). Since tan(-π/4)= -1, so tan(-0.9227)= tan(-π/4 -0.1373)= [tan(-π/4) + tan(-0.1373)] / [1 - tan(-π/4)tan(-0.1373)]≈[-1 -0.138]/[1 - (-1)(-0.138)]≈-1.138/(1 -0.138)≈-1.138/0.862≈-1.32, which is not -1, so something's wrong here. Wait, but according to our earlier formula, tan S should be exactly -1, so why does the approximate calculation give a different value?Because we used approximate values for x₁, x₂, x₃. If we use exact roots, the formula must hold. So maybe even though our approximate sum is about -0.9227, which has a tangent of≈-1.32, the exact sum S has tan S = -1. So there's a contradiction here unless our approximate calculation is missing something.Wait, perhaps the exact value of S is 3π/4, but that's in the second quadrant. But our approximate sum is in the fourth quadrant. So how can this be?Wait, maybe the individual arctans are not all in the principal branch? No, arctan is defined to give values between -π/2 and π/2. So arctan x₁ and arctan x₂ are negative, arctan x₃ is positive. So their sum is S = arctan x₁ + arctan x₂ + arctan x₃. Since arctan x₁ and arctan x₂ are both negative, their sum is more negative than arctan x₃ is positive. So overall, depending on the values, S could be negative or positive. However, according to the approximate sum, S is negative.But if tan S = -1, then possible values of S are -π/4, 3π/4, 7π/4, etc. But S is approximately -0.9227, which is -π/4 -0.137 radians. But there's a formula discrepancy here. Wait, maybe this is a trick question where the sum is actually -π/4, but the approximation is misleading? Let's check with exact values.Wait, if tan S = -1, then S = -π/4 + kπ. But we need to determine k. Since the approximate sum is around -0.925, which is approximately -π/4 -0.137, so k=0 would give S=-π/4≈-0.785, which is more positive than our approximate sum. If k=-1, S=-π/4 -π≈-3.927, which is way more negative. So neither. Therefore, something is wrong. Alternatively, maybe the formula gives tan S=-1, but S is not in the principal branch. Wait, but the formula for tan(A+B+C) is valid regardless of the quadrant. So S can be any angle such that tan S=-1, which are S = -π/4 +kπ. But depending on the actual value of the sum, which is approximately -0.925, which is between -π/2 and 0, so k=0. Therefore, S= -π/4. But how? The approximate sum is -0.925, which is less than -π/4≈-0.785. So unless my approximation is off.Wait, let's get more accurate estimates of the roots.Let's try to find x₁ more accurately. Since x₁ is between -4 and -3, and f(-4) = -14, f(-3)=6. Let's use linear approximation between x=-4 and x=-3.f(-4)=-14, f(-3)=6. So slope is 6 - (-14)=20 over 1 unit. To find x where f(x)=0: let's assume f(x) increases linearly. So from x=-4 to x=-3, f(x) increases by 20. So to go from -14 to 0, need to cover 14/20=0.7 units from x=-4. So x₁≈-4 +0.7≈-3.3. Let's check f(-3.3):(-3.3)^3 -17*(-3.3) -18.First, (-3.3)^3= -35.937-17*(-3.3)=56.1So total: -35.937 +56.1 -18 = (56.1 -35.937)=20.163; 20.163 -18=2.163. So f(-3.3)=2.163. Hmm, positive. So need to go further left. Since f(-4)=-14, f(-3.3)=2.163. So root is between -4 and -3.3. Let's do a better approximation.Let’s try x=-3.5:f(-3.5)=(-3.5)^3 -17*(-3.5) -18= -42.875 +59.5 -18= (59.5 -42.875)=16.625 -18= -1.375. So f(-3.5)= -1.375.f(-3.5)= -1.375, f(-3.3)=2.163. So between x=-3.5 and x=-3.3. Let's find where f(x)=0.Let’s use linear approximation between x=-3.5 and x=-3.3.f(-3.5)= -1.375f(-3.3)=2.163Difference in f: 2.163 - (-1.375)=3.538 over 0.2 units of x.To cover 1.375 to reach 0, need (1.375 /3.538)*0.2≈ (0.388)*0.2≈0.0776. So x≈-3.5 +0.0776≈-3.4224. Let's check f(-3.4224):x=-3.4224x³: (-3.4224)^3≈-3.4224*3.4224*3.4224≈-3.4224*(11.711)≈-40.1-17x≈-17*(-3.4224)=58.1808-18.Total≈-40.1 +58.1808 -18≈0.0808. Close to zero. So maybe x₁≈-3.4224. Let's use a better approximation.Take x=-3.43:x³ = (-3.43)^3 ≈-40.359-17x≈58.31Total: -40.359 +58.31 -18≈-40.359 +40.31≈-0.049. So f(-3.43)≈-0.049.x=-3.42:x³≈(-3.42)^3≈-3.42*3.42*3.42≈-3.42*(11.6964)≈-40.0-17*(-3.42)=58.14Total: -40.0 +58.14 -18=0.14. So f(-3.42)=0.14.Therefore, the root x₁ is between -3.43 and -3.42. Using linear approximation between x=-3.43 (f=-0.049) and x=-3.42 (f=0.14). The difference in f is 0.14 - (-0.049)=0.189 over 0.01 x. To reach zero from x=-3.43, need 0.049/0.189≈0.259 of the interval. So x≈-3.43 +0.259*0.01≈-3.43 +0.00259≈-3.4274. So x₁≈-3.4274.Similarly, find x₃ between4 and5.f(4)=64 -68 -18= -22, f(5)=125 -85 -18=22. So the root is between4 and5.Let's approximate x₃. Let's try x=4.5:f(4.5)=91.125 -76.5 -18= -3.375.f(4.5)= -3.375. f(5)=22. So between4.5 and5.Take x=4.6:4.6³=97.33617*4.6=78.2f(4.6)=97.336 -78.2 -18=1.136.So f(4.6)=1.136. f(4.5)= -3.375. So root between4.5 and4.6.Linear approximation:From x=4.5 (f=-3.375) to x=4.6 (f=1.136). Difference in f=1.136 -(-3.375)=4.511 over 0.1 x.To cover 3.375, need 3.375/4.511≈0.748 of the interval. So x≈4.5 +0.748*0.1≈4.5 +0.0748≈4.5748. Check f(4.5748):x=4.5748x³≈4.5748³≈4.5748*4.5748*4.5748. Let's compute step by step:4.5748*4.5748≈20.92. Then 20.92*4.5748≈95.73.17x≈17*4.5748≈77.7716f(x)=95.73 -77.7716 -18≈95.73 -95.7716≈-0.0416. So f(4.5748)≈-0.0416.x=4.575:x³≈4.575^3. 4.575*4.575=20.9306. 20.9306*4.575≈95.778.17x=17*4.575≈77.775.f(x)=95.778 -77.775 -18≈0.003. So f(4.575)=0.003. Therefore, x₃≈4.575.So x₃≈4.575, x₁≈-3.4274. Then x₂= -x₁ -x₃≈3.4274 -4.575≈-1.1476. So x₂≈-1.1476.Therefore, x₂ is≈-1.1476, which is between -2 and -1, as we thought earlier. So integer part is -2 for x₂.Now, arctan x₁ + arctan x₂ + arctan x₃≈arctan(-3.4274)+arctan(-1.1476)+arctan(4.575).Compute each arctan:arctan(-3.4274)≈-1.287 radians (since arctan(-3.4274)= -arctan(3.4274). arctan(3.4274)≈1.287 radians.arctan(-1.1476)≈-0.854 radians.arctan(4.575)≈1.355 radians.Sum≈-1.287 -0.854 +1.355≈(-2.141) +1.355≈-0.786 radians.Which is≈-0.786 radians, which is≈-45 degrees, since π/4≈0.785 radians. So -0.786≈-π/4. Therefore, the exact value is -π/4. But wait, according to our approximate calculation, the sum is≈-π/4. But the approximate sum of the approximate roots gives≈-π/4. So why the confusion earlier? Because with the approximated x₂≈-1.1476, which is more accurately placed, the sum is indeed≈-π/4. Therefore, the exact value must be -π/4. But wait, tan S = -1, so S can be -π/4 +kπ. Since the approximate sum is≈-π/4, and since the tangent is periodic with period π, the exact sum must be -π/4. Therefore, the answer is -π/4. But arctan returns principal values, but the sum could be adjusted by multiples of π. However, given the approximate sum is around -π/4, and the formula suggests tan S=-1, it's reasonable to conclude that S=-π/4.But wait, the problem says "Find the value of arctan x₁ + arctan x₂ + arctan x₃". If the sum is -π/4, but arctan values are all in (-π/2, π/2), how does the sum end up as -π/4?Wait, but if two of the arctans are negative and one is positive, their sum can be within (-3π/2, 3π/2). However, in reality, since each arctan is between -π/2 and π/2, the maximum sum would be less than 3π/2 and the minimum greater than -3π/2. But in our case, the sum is approximately -π/4, which is within (-π/2, π/2), so it's the principal value. Therefore, the sum is indeed -π/4. But wait, according to the exact calculation, tan S = -1, and S≈-π/4. So the answer is -π/4. However, arctan values are typically taken as principal values, but the sum could technically be -π/4 +kπ. But given the approximate sum is around -π/4, which is within the principal branch, the answer is -π/4. However, -π/4 is equivalent to 7π/4 in terms of tangent, but since the sum is in the fourth quadrant, the answer is -π/4. But we need to confirm if there's a formula that directly gives this.Alternatively, let's consider the identity:If tan S = -1, then S = arctan(-1) = -π/4, but since the tangent function has a period of π, we have S = -π/4 +kπ. However, to determine the correct k, we need to look at the individual arctans.Given that x₁≈-3.4274, arctan(x₁)≈-1.287 radians.x₂≈-1.1476, arctan(x₂)≈-0.854 radians.x₃≈4.575, arctan(x₃)≈1.355 radians.Sum≈-1.287 -0.854 +1.355≈-0.786≈-π/4≈-0.785 radians.Therefore, the exact sum S is exactly -π/4. Therefore, the answer is -π/4.But let's check with the exact values:Given that tan S = -1, and S≈-π/4. So unless there is a reason for the sum to be another angle, such as π - π/4=3π/4, but that would be in a different quadrant. However, since all the individual arctans are within (-π/2, π/2), their sum must be within (-3π/2, 3π/2). But with two negative terms and one positive term, the sum is in (-π/2 -π/2 +0, 0 +0 +π/2)= (-π, π/2). Our sum is≈-π/4, which is within (-π, π/2), and is in the fourth quadrant. Therefore, the correct value is S=-π/4.Therefore, the answer to part (2) is -π/4. But wait, the problem says "Find the value", and arctan sums can sometimes have a modulus consideration. But since we've verified through multiple approaches that the sum is -π/4, and the tangent of this sum is -1, which matches the formula derived from Vieta's, it must be correct.Therefore, the answers are:(1) The integer part of x₂ is boxed{-2}.(2) The value of arctan x₁ + arctan x₂ + arctan x₃ is boxed{-dfrac{pi}{4}}.Final Answer(1) The integer part of ( x_2 ) is (boxed{-2}).(2) The value of ( arctan x_1 + arctan x_2 + arctan x_3 ) is (boxed{-dfrac{pi}{4}}).</think>Given the cubic equation (x^3 - 17x - 18 = 0) with roots (x_1), (x_2), and (x_3), where (x_1) is between (-4) and (-3), and (x_3) is between (4) and (5):1. Finding the integer part of (x_2): Using Vieta's formulas for the cubic equation: - The sum of the roots: (x_1 + x_2 + x_3 = 0) - The product of the roots: (x_1 x_2 x_3 = 18) - The sum of the products of the roots taken two at a time: (x_1 x_2 + x_1 x_3 + x_2 x_3 = -17) Since (x_1) is between (-4) and (-3) and (x_3) is between (4) and (5), we find (x_2) using the sum of the roots: [ x_2 = -x_1 - x_3 ] Given the intervals for (x_1) and (x_3), (x_2) ranges between (-2) and (0). By evaluating the function (f(x) = x^3 - 17x - 18) at intermediate points, we determine that (x_2) lies between (-2) and (-1). Therefore, the integer part of (x_2) is (-2).2. Finding the value of (arctan x_1 + arctan x_2 + arctan x_3): Using the tangent addition formula for three angles: [ tan(arctan x_1 + arctan x_2 + arctan x_3) = frac{x_1 + x_2 + x_3 - x_1 x_2 x_3}{1 - (x_1 x_2 + x_1 x_3 + x_2 x_3)} ] Substituting Vieta's formulas: - (x_1 + x_2 + x_3 = 0) - (x_1 x_2 + x_1 x_3 + x_2 x_3 = -17) - (x_1 x_2 x_3 = 18) We get: [ tan(arctan x_1 + arctan x_2 + arctan x_3) = frac{0 - 18}{1 - (-17)} = frac{-18}{18} = -1 ] The angle whose tangent is (-1) and lies in the appropriate quadrant (considering the approximate values of the arctans) is (-frac{pi}{4}). Final Answers1. The integer part of (x_2) is (boxed{-2}).2. The value of (arctan x_1 + arctan x_2 + arctan x_3) is (boxed{-dfrac{pi}{4}}).,<think>Okay, let's tackle this problem step by step. It's about a cubic equation and some properties of its roots. The equation is given as (x^3 - 17x - 18 = 0), and the roots are (x_1), (x_2), (x_3). We know that (x_1) is between -4 and -3, and (x_3) is between 4 and 5. The questions are: (1) Find the integer part of (x_2), and (2) Find the value of (arctan x_1 + arctan x_2 + arctan x_3).Starting with part (1). The integer part of (x_2) means the greatest integer less than (x_2). Since (x_1), (x_2), (x_3) are roots of the cubic equation, maybe we can use Vieta's formula here. Vieta's formulas relate the coefficients of a polynomial to sums and products of its roots. For a cubic equation (x^3 + ax^2 + bx + c = 0), the sum of the roots is (-a), the sum of the products of the roots taken two at a time is (b), and the product of the roots is (-c).Our equation is (x^3 - 17x - 18 = 0). Comparing to the general form, (a = 0), (b = -17), (c = -18). So, applying Vieta's formulas:1. (x_1 + x_2 + x_3 = -a = 0)2. (x_1x_2 + x_1x_3 + x_2x_3 = b = -17)3. (x_1x_2x_3 = -c = 18)Given that the sum of the roots is zero. So (x_1 + x_2 + x_3 = 0). We know the approximate ranges for (x_1) and (x_3): (x_1) is between -4 and -3, (x_3) is between 4 and 5. Let me write that:(-4 < x_1 < -3)(4 < x_3 < 5)Since the sum is zero, (x_2 = - (x_1 + x_3)). So substituting the ranges for (x_1) and (x_3):Let's compute the possible values of (x_1 + x_3). The minimum possible sum of (x_1 + x_3) is when (x_1) is as small as possible and (x_3) is as small as possible: (-4 + 4 = 0). The maximum possible sum is when (x_1) is as large as possible and (x_3) is as large as possible: (-3 + 5 = 2). Therefore, (0 < x_1 + x_3 < 2), so (x_2 = - (x_1 + x_3)) implies that (-2 < x_2 < 0). Therefore, the integer part of (x_2) is either -2, -1, or 0? Wait, but if x2 is between -2 and 0, then the integer part (which is the floor function) would be -2 if x2 is between -2 and -1, -1 if x2 is between -1 and 0. So we need to narrow down the value of (x_2).But maybe we can get a better estimate. Let's see. Let's take the midpoints. Suppose (x_1 ≈ -3.5) and (x_3 ≈ 4.5), then (x_2 ≈ -(-3.5 + 4.5) = -1). But maybe this is too rough. Alternatively, we can use the fact that the cubic equation can be graphed to approximate the roots.Alternatively, since the equation is (x^3 -17x -18 =0), maybe we can find approximate values for (x_1), (x_2), (x_3).Wait, but the problem gives us the intervals for (x_1) and (x_3). So maybe with those intervals, and the relation (x_1 + x_2 + x_3 =0), we can narrow down (x_2).Wait, but the problem says part (1) is to find the integer part of (x_2). Since the possible range for (x_2) is between -2 and 0, as we saw, but need to be more precise. Let's try to compute possible values.If (x_1) is between -4 and -3, and (x_3) is between 4 and 5, then:The minimum value of (x_1 + x_3) is (-4) + 4 = 0, and maximum is (-3) +5=2. So (x_2) is between -2 and 0. But depending on the actual values of (x_1) and (x_3), the sum could be such that (x_2) is in different parts of that interval.But perhaps we can use another Vieta formula. The sum of products: (x_1x_2 + x_1x_3 + x_2x_3 = -17). Let me see. Let's denote S = x1 + x2 + x3 = 0. Let’s denote P = x1x2x3 = 18.Alternatively, maybe we can express (x_1x_2 + x_1x_3 + x_2x_3 = -17). Let me rewrite this as (x_1(x_2 + x_3) + x_2x_3 = -17). But since (x_2 + x_3 = -x_1), so substituting:(x_1(-x_1) + x_2x_3 = -17)Which simplifies to:(-x_1^2 + x_2x_3 = -17)Therefore, (x_2x_3 = x_1^2 -17)Similarly, since (x_1x_2x_3 =18), so (x_2x_3 =18 / x_1)Therefore, equating the two expressions for (x_2x_3):(x_1^2 -17 = 18 / x_1)Multiply both sides by (x_1) (assuming (x_1 neq 0), which it isn't because x1 is between -4 and -3):(x_1^3 -17x_1 -18 =0)Wait, but this is the original equation. So this doesn't help. Hmm. Maybe we can use some other approach.Alternatively, perhaps approximate the roots numerically.Given the equation (x^3 -17x -18 =0). Let's see:First, let's check the given intervals for (x_1) and (x_3):For (x_1) between -4 and -3:Let's test x = -4: (-4)^3 -17*(-4) -18 = -64 +68 -18 = (-64 +68)=4; 4-18=-14 <0x = -3: (-3)^3 -17*(-3) -18 = -27 +51 -18 = (-27 +51)=24; 24-18=6 >0So the equation crosses from negative to positive between x=-4 and x=-3, hence a root there.Similarly for x=4: 64 -68 -18= (64-68)= -4; -4-18=-22 <0x=5: 125 -85 -18=125-103=22>0, so root between 4 and5.Therefore, the roots are in those intervals as given. Now, the third root (x_2) is somewhere else. Since the cubic equation has three real roots? Wait, how do we know?Alternatively, maybe there are two complex roots and one real root? But the problem states three roots x1, x2, x3, so all real. Let me check the discriminant of the cubic equation.The discriminant D of a cubic equation (x^3 + ax^2 + bx + c =0) is given by D = 18abc -4a^3c + a^2b^2 -4b^3 -27c^2.In our case, equation is (x^3 +0x^2 -17x -18=0), so a=0, b=-17, c=-18.Plug into discriminant formula:D = 18*0*(-17)*(-18) -4*0^3*(-18) +0^2*(-17)^2 -4*(-17)^3 -27*(-18)^2Simplify term by term:First term: 0Second term: 0Third term: 0Fourth term: -4*(-17)^3 = -4*(-4913)= 19652Fifth term: -27*(324) = -8748So total D = 19652 -8748 = 10904Since D >0, all roots are real and distinct. So three real roots.So, we have three real roots. So x2 is the remaining real root. Since sum of roots is zero, and x1 is negative, x3 is positive, so x2 must be the other root.Now, to approximate x2. Since the integer part is required, perhaps we can use intermediate value theorem to approximate x2.Let me check the value of the function at some integer points between -2 and 0.First, check x= -2:f(-2) = (-8) -17*(-2) -18 = -8 +34 -18= 8 >0x=-1:f(-1)= (-1) -17*(-1) -18= -1 +17 -18= -2 <0x=0:f(0)=0 -0 -18= -18 <0Wait, hold on. Wait, the function at x=-2 is 8, at x=-1 is -2, and at x=0 is -18. Wait, but if x2 is between -2 and 0, but f(-2)=8, f(-1)=-2, f(0)=-18. So there's a root between x=-2 and x=-1 because the function changes sign from positive to negative. Therefore, x2 is between -2 and -1. Therefore, the integer part of x2 is -2.Wait, but let's confirm.Wait, the cubic equation has three real roots. We have roots at x1 (-4 to -3), x2, and x3 (4 to5). Since f(-4)= -64 -17*(-4) -18= -64 +68 -18= -14f(-3)= -27 -17*(-3) -18= -27 +51 -18=6So root x1 between -4 and -3.Then, f(-2)=8, f(-1)=-2, f(0)=-18, so between -2 and -1, the function goes from 8 to -2, so crosses zero there, that's x2.Then between x=4 and5, as checked before, f(4)= -22, f(5)=22, so root x3 there.Therefore, x2 is between -2 and -1, so integer part is -2. Therefore, answer to (1) is -2.But the problem says "the integer part of x2". The integer part is the floor function, which is the greatest integer less than or equal to x2. Since x2 is between -2 and -1, the floor of x2 is -2. So part (1) is -2.Now part (2): arctan x1 + arctan x2 + arctan x3.Hmm. Need to find the sum of arctans of the roots. Let's think about properties of arctangent. The formula for arctan a + arctan b = arctan((a + b)/(1 - ab)) + kπ, depending on the quadrant. But here we have three terms, so maybe we can use some identity.Alternatively, perhaps there is a relationship between the roots that can help. Since x1 + x2 +x3=0. Let's denote S = arctan x1 + arctan x2 + arctan x3.I recall that if three numbers a, b, c satisfy a + b + c = abc, then arctan a + arctan b + arctan c = π. Wait, is that right? Let me check.Suppose a, b, c >0, and a + b + c = abc, then arctan a + arctan b + arctan c = π. Yes, that is a known identity. But in our case, the roots x1, x2, x3 satisfy x1 + x2 + x3 =0 and x1x2x3=18. So not sure if that identity applies here.Alternatively, perhaps use the tangent addition formula. Let me attempt to compute tan(S) where S = arctan x1 + arctan x2 + arctan x3.Using tan(A + B + C) formula. Let me first compute tan(arctan x1 + arctan x2 + arctan x3). Let’s denote A = arctan x1, B = arctan x2, C = arctan x3. So tan(A + B + C) = [tan A + tan B + tan C - tan A tan B tan C] / [1 - tan A tan B - tan B tan C - tan C tan A]But tan A = x1, tan B = x2, tan C = x3. So plug in:tan(S) = [x1 + x2 + x3 - x1x2x3] / [1 - (x1x2 + x2x3 + x3x1)]But from Vieta:x1 + x2 + x3 =0x1x2 + x2x3 + x3x1 = -17x1x2x3=18Therefore, substitute:tan(S) = [0 - 18] / [1 - (-17)] = (-18)/(1 +17) = (-18)/18 = -1Therefore, tan(S) = -1. Therefore, S = arctan(-1) + kπ. But arctan(-1) is -π/4, but since the sum of arctans can be in different quadrants.But we need to find S = arctan x1 + arctan x2 + arctan x3. Let's consider the ranges of each arctan.Given that x1 is between -4 and -3, so arctan x1 is between arctan(-4) and arctan(-3). Arctan of a negative number is negative, so arctan x1 is between -arctan 4 and -arctan3, which is approximately between -1.3258 and -1.2490 radians (since arctan3 ≈1.2490, arctan4≈1.3258). So arctan x1 is approximately -1.3 radians.x2 is between -2 and -1, so arctan x2 is between arctan(-2)≈-1.1071 and arctan(-1)= -π/4≈-0.7854 radians.x3 is between 4 and5, so arctan x3 is between arctan4≈1.3258 and arctan5≈1.3734 radians.So adding them up: arctan x1 is ≈-1.3, arctan x2≈-0.9, arctan x3≈1.35. Sum≈-1.3 -0.9 +1.35≈-0.85 radians. But tan(S)= -1, so S could be -π/4 or 3π/4, but -0.85 is approximately -π/4≈-0.785, but -0.85 is a bit less than that. Wait, but this is confusing.Wait, tan(S) = -1, so S = -π/4 + kπ. But the actual sum of the arctans is some real number. Let's compute approximate values:Compute approximate arctan x1:x1≈-3.5 (midpoint of -4 and -3). arctan(-3.5)= -arctan(3.5). Arctan3.5≈1.2925 radians, so arctan x1≈-1.2925x2≈-1.5 (midpoint of -2 and -1). arctan(-1.5)= -arctan1.5≈-0.9828x3≈4.5. arctan4.5≈1.3526Sum≈-1.2925 -0.9828 +1.3526≈-0.9227 radians.Now, tan(-0.9227)= tan(-0.9227 + π)=tan(2.2189)=≈-1. Because tan(π - θ) = -tanθ. Wait, but tan(-0.9227)= tan(-0.9227 + π)=tan(2.2189)=tan(π -0.9227)= -tan(0.9227). Since 0.9227*180/π≈53 degrees, tan(0.9227)≈1.333, so tan(-0.9227)≈-1.333. Wait, that contradicts the previous result that tan(S)= -1.Wait, but according to the formula, tan(S)= -1, so S should be -π/4 +kπ. But our approximate sum is -0.9227 radians, which is approximately -53 degrees. But -π/4 is -45 degrees. So there is a discrepancy here. This suggests that perhaps the exact value is -π/4, but due to approximation errors, our numerical estimate is close but not exact.Alternatively, perhaps the exact value is 3π/4. Let's check:If S = 3π/4 ≈2.356 radians. tan(3π/4)= -1. But our approximate sum is around -0.92 radians, which is not 3π/4. Alternatively, maybe S = -π/4. But our approximate sum is -0.92, which is more negative than -π/4≈-0.785.But wait, perhaps the actual sum is -π/4. Let's see. If S = arctan x1 + arctan x2 + arctan x3, and tan(S)= -1, then S = -π/4 +kπ. The question is, which multiple of π to take.Given that x1 is negative, x2 is negative, x3 is positive. Let's analyze each arctan:arctan x1 is negative (since x1 is negative), arctan x2 is negative (x2 is negative), arctan x3 is positive (x3 is positive). So the total sum S is negative + negative + positive. Depending on the magnitudes, the sum could be negative or positive.But in our approximate calculation, the sum was around -0.92 radians, which is approximately -52.7 degrees. But if S must be congruent to -π/4 modulo π, so possible values are -π/4, 3π/4, 7π/4, etc. But the principal value of arctan is between -π/2 and π/2. However, the sum of three arctans can be outside this range.But since two of the terms are negative and one is positive, the total sum could be between:Minimum possible sum: arctan(-4) + arctan(-2) + arctan4 ≈ (-1.3258) + (-1.1071) +1.3258≈-1.1071 radians≈-63.4 degreesMaximum possible sum: arctan(-3) + arctan(-1) + arctan5≈(-1.2490)+ (-0.7854)+1.3734≈-0.6610 radians≈-37.8 degreesSo the sum S is between approximately -1.1071 and -0.6610 radians. The only angle in this interval that satisfies tan(S) = -1 is -π/4≈-0.7854 radians. Because tan(-π/4)= -1. So perhaps the exact value is -π/4, but the approximate calculation was around -0.92, which is close but not exact. Wait, but maybe my approximations are too rough.Wait, but according to the formula, tan(S)= -1. Therefore, S must be an angle whose tangent is -1, which occurs at -π/4 +kπ. The question is, which one is it?Given that S is the sum of two negative arctans and one positive. Let's think about the actual values.If x1 ≈ -3.5, x2≈-1.5, x3≈4.5.Compute arctan(-3.5) ≈ -1.2925arctan(-1.5)≈-0.9828arctan(4.5)≈1.3526Sum≈-1.2925 -0.9828 +1.3526≈-0.9227 radians. Which is approximately -52.8 degrees.But tan(-0.9227)= tan(-0.9227)≈-1.333, which is not -1. But according to our earlier formula, tan(S)= -1. This contradiction suggests that either the approximation is too rough, or there is an exact value.Wait, but the formula is exact: tan(S) = -1. So S must be -π/4 +kπ. So S is congruent to -π/4 modulo π. But the actual numerical value is approximately -0.9227, which is equal to -π/4 - (0.9227 -0.7854)= -π/4 -0.1373≈-0.7854 -0.1373≈-0.9227. So it's -π/4 minus approximately 0.1373 radians. So how can that be?Wait, but according to the formula, tan(S)= -1 exactly. But if S=arctan x1 + arctan x2 + arctan x3, then tan(S)= -1 exactly, so S must be -π/4 +kπ. However, the actual sum S is a specific number. So the sum is equal to -π/4 modulo π, but we need to determine the exact value.But given that the sum is between -1.1071 and -0.6610 radians, which is between approximately -63.4 degrees and -37.8 degrees. The only angle in this interval with tan(S)= -1 is -π/4 (-45 degrees). But -45 degrees is -0.7854 radians, which is within the interval (-1.1071, -0.6610). So even though our approximate sum is around -0.9227, which is outside of (-0.7854, -0.6610), but that's only an approximation. The exact value must be -π/4, but let me check.Wait, perhaps there is an exact relation here. Let me consider that x1 +x2 +x3=0 and x1x2x3=18. Maybe there's an identity involving arctans when sum of variables is zero.Alternatively, consider complex numbers. Let's think of the formula for the argument of a complex number. If we have three complex numbers with arguments arctan x1, arctan x2, arctan x3, then the sum of arguments is the argument of the product. But this might not apply here. Wait, but if we consider complex numbers z1 =1 + ix1, z2=1 +ix2, z3=1 +ix3. Then the arguments of z1, z2, z3 are arctan x1, arctan x2, arctan x3 respectively. Then the argument of z1 z2 z3 would be the sum of the arguments. But the product z1 z2 z3 would be (1 +ix1)(1 +ix2)(1 +ix3). Let's compute this product.Expand the product:First multiply (1 +ix1)(1 +ix2) =1 +i(x1 +x2) +i^2 x1x2 =1 +i(x1 +x2) -x1x2Then multiply by (1 +ix3):[1 -x1x2 +i(x1 +x2)] [1 +ix3] = (1 -x1x2)(1) + (1 -x1x2)(ix3) +i(x1 +x2)(1) +i(x1 +x2)(ix3)Simplify term by term:1 -x1x2 +i x3 (1 -x1x2) +i(x1 +x2) +i^2 x3(x1 +x2)=1 -x1x2 +i x3 -i x1x2x3 +i x1 +i x2 -x3(x1 +x2)Combine like terms:Real parts: 1 -x1x2 -x3x1 -x3x2Imaginary parts: x3 +x1 +x2 -x1x2x3But from Vieta:x1 +x2 +x3=0 ⇒ x3 = -x1 -x2x1x2 +x1x3 +x2x3= -17x1x2x3=18Let me substitute x3 = -x1 -x2 into real parts:Real parts: 1 -x1x2 -x3(x1 +x2) =1 -x1x2 -(-x1 -x2)(x1 +x2)=1 -x1x2 + (x1 +x2)^2Expand (x1 +x2)^2 =x1^2 +2x1x2 +x2^2So Real parts:1 -x1x2 +x1^2 +2x1x2 +x2^2=1 +x1^2 +x2^2 +x1x2Imaginary parts: x3 +x1 +x2 -x1x2x3= 0 -x1x2x3= -18 (since x1x2x3=18)Wait, because x3 +x1 +x2=0, so first three terms are 0, and the last term is -x1x2x3= -18.Therefore, the product z1 z2 z3= [1 +x1^2 +x2^2 +x1x2] +i*(-18)Therefore, the argument of z1 z2 z3 is arctan( -18 / (1 +x1^2 +x2^2 +x1x2) )But the argument of z1 z2 z3 is equal to the sum of the arguments of z1, z2, z3, which is S=arctanx1 + arctanx2 + arctanx3.Therefore, S= arctan( -18 / (1 +x1^2 +x2^2 +x1x2) ) +kπ.But we also know that tan(S)= -1, so:-18 / (1 +x1^2 +x2^2 +x1x2) = -1 ⇒ 18 / (1 +x1^2 +x2^2 +x1x2) =1 ⇒ 1 +x1^2 +x2^2 +x1x2=18.So, need to check whether 1 +x1^2 +x2^2 +x1x2=18.But can we express x1^2 +x2^2 +x1x2 in terms of Vieta's formulas?We know that x1 +x2 +x3=0 ⇒ x3= -x1 -x2.Then x1^2 +x2^2 +x1x2= x1^2 +x2^2 +x1x2.Also, from x1 +x2 +x3=0, squaring both sides: x1^2 +x2^2 +x3^2 +2(x1x2 +x1x3 +x2x3)=0From Vieta, x1x2 +x1x3 +x2x3= -17.Therefore:x1^2 +x2^2 +x3^2 +2*(-17)=0 ⇒ x1^2 +x2^2 +x3^2=34.But x3= -x1 -x2, so x3^2=(x1 +x2)^2 =x1^2 +2x1x2 +x2^2.Therefore, substituting back:x1^2 +x2^2 +x1^2 +2x1x2 +x2^2=34 ⇒2x1^2 +2x2^2 +2x1x2=34 ⇒x1^2 +x2^2 +x1x2=17.Therefore, 1 +x1^2 +x2^2 +x1x2=1 +17=18. Which matches the previous equation.Therefore, arctan( -18 /18 )= arctan(-1)= -π/4.Therefore, the argument S= arctanx1 +arctanx2 +arctanx3= -π/4 +kπ. But we need to determine the correct k.Since the product z1 z2 z3 has a negative imaginary part and positive real part (since 1 +x1^2 +x2^2 +x1x2=18, which is positive, and imaginary part is -18), the argument is in the fourth quadrant (positive real, negative imaginary). Therefore, the principal value of the argument is between -π/2 and 0. Therefore, S= -π/4.But earlier approximation suggested the sum is around -0.92 radians, which is approximately -52 degrees, more negative than -π/4≈-45 degrees. However, according to the exact calculation, the sum S is -π/4. This discrepancy arises because when we take the principal value of the argument, which is between -π and π, but in this case, since the complex number z1 z2 z3 is in the fourth quadrant, the argument is indeed -π/4. However, the individual arctans are each between -π/2 and π/2, and their sum could be outside this range, but the total argument is adjusted by adding multiples of π.Wait, but in complex analysis, the argument of a complex number is modulo 2π. However, when we compute the sum of arguments of z1, z2, z3, it's possible that the total argument exceeds π or is less than -π, but the principal value is adjusted accordingly.However, in our case, the product z1 z2 z3 is (1 +ix1)(1 +ix2)(1 +ix3)=18 -18i. Wait, wait:Earlier computation showed that the product has real part 18 and imaginary part -18. Wait, no:Wait, real part was 1 +x1^2 +x2^2 +x1x2=18, and imaginary part is -18. So the product is 18 -18i. Therefore, the complex number 18 -18i lies in the fourth quadrant, with argument arctan(-18/18)= arctan(-1)= -π/4. Therefore, the principal value of the argument is indeed -π/4.But the sum of the arguments of z1, z2, z3 is equal to the argument of the product, which is -π/4. However, each individual argument (arctan x1, arctan x2, arctan x3) is between -π/2 and π/2, but their sum can be outside that interval. However, the argument of the product is equivalent to the sum modulo 2π. In this case, since the product is 18 -18i, the argument is -π/4, which is equivalent to 7π/4. However, since we are considering the principal value, which is between -π and π, it is -π/4.Therefore, the sum S= arctanx1 +arctanx2 +arctanx3= -π/4.But this contradicts our approximate calculation. However, the exact result from the complex number approach gives S= -π/4, so that must be the correct answer. Therefore, part (2) is -π/4. But arctangent sum formulas usually give results modulo π, but in this case, due to the specific values, it's exactly -π/4.Wait, but the problem says "Find the value of arctan x1 + arctan x2 + arctan x3". If it's exactly -π/4, then that's the answer. But let's check again.Given that tan(S)= -1, and the product z1 z2 z3=18 -18i, whose argument is -π/4. Therefore, the sum of the arguments of z1, z2, z3 is -π/4. However, the arguments of z1, z2, z3 are not exactly the same as arctan x1, arctan x2, arctan x3. Wait, z1=1 +ix1, so the argument is arctan(x1 /1 )= arctanx1, same for z2, z3. Therefore, the argument of the product is indeed the sum of the individual arguments, which is S=arctanx1 + arctanx2 + arctanx3. Since the product is 18 -18i, whose argument is -π/4, then S= -π/4 +2πk. But the principal value of the argument is between -π and π. Therefore, S= -π/4 is the correct value.But when I approximated the sum using x1≈-3.5, x2≈-1.5, x3≈4.5, I got around -0.9227 radians≈-52.8 degrees, which is not -45 degrees. But since the exact answer is -π/4, which is -45 degrees, perhaps the approximate calculation is not precise enough, and the exact value is indeed -π/4.Therefore, the answer to part (2) is -π/4. But usually, such sums are given in terms of positive angles. Wait, but -π/4 is equivalent to 7π/4, but since we are to present it as a value, likely -π/4 is acceptable, but maybe it's expressed as a positive angle. However, depending on the convention. The problem doesn't specify, but since it's the sum of three arctangents, which are angles whose tangents are x1, x2, x3. Since x1 and x2 are negative, their arctans are negative, and x3 is positive, its arctan is positive. The sum is negative. However, the problem asks for the value, so it should be -π/4.Alternatively, maybe there's a mistake here. Let me verify with another approach.Let me consider that S = arctanx1 + arctanx2 + arctanx3 = -π/4.But let's use another formula. We have tan(S) = -1. So possible solutions are S = -π/4 +kπ. To determine k, we need to know the actual value.Given that:arctan x1 is between -1.3258 and -1.2490 (≈-75 to -71 degrees)arctan x2 is between -1.1071 and -0.7854 (≈-63.4 to -45 degrees)arctan x3 is between 1.3258 and 1.3734 (≈75.7 to 78.7 degrees)So summing these ranges:Minimum total: (-1.3258) + (-1.1071) +1.3258≈-1.1071 radians≈-63.4 degreesMaximum total: (-1.2490) + (-0.7854) +1.3734≈-0.6610 radians≈-37.8 degreesSo the sum is between approximately -63.4 degrees and -37.8 degrees, which is between -1.107 radians and -0.661 radians. The angle -π/4 is -0.785 radians, which is within this interval. Therefore, S= -π/4 is the correct value because tan(S)= -1 and S is within the required interval. Therefore, the answer is -π/4.But angles can also be represented as positive angles by adding 2π. But since -π/4 is within the principal value range of -π to π, there is no need to adjust. Therefore, the value is -π/4.But the problem says "Find the value", so maybe the answer is -π/4. However, usually, such problems expect a positive angle, but in this case, since the sum is negative, -π/4 is appropriate.Alternatively, maybe there's a different approach. Let's suppose that the three roots x1, x2, x3 satisfy certain relationships that make the sum of arctans equal to -π/4. Given that the product of the roots is 18 and their sum is zero, perhaps this is a constructed identity.Therefore, after careful consideration, part (2) is -π/4.Final Answer(1) The integer part of (x_2) is boxed{-2}.(2) The value of (arctan x_1 + arctan x_2 + arctan x_3) is boxed{-dfrac{pi}{4}}.</think>Given the cubic equation (x^3 - 17x - 18 = 0) with roots (x_1), (x_2), and (x_3), where (-4 < x_1 < -3) and (4 < x_3 < 5):1. Finding the integer part of (x_2): Using Vieta's formulas: - The sum of the roots: (x_1 + x_2 + x_3 = 0) - Given the intervals for (x_1) and (x_3), we approximate the range of (x_2): - The minimum value of (x_1 + x_3) is (0) (when (x_1 = -4) and (x_3 = 4)) - The maximum value of (x_1 + x_3) is (2) (when (x_1 = -3) and (x_3 = 5)) - Therefore, (-2 < x_2 < 0) - Using the Intermediate Value Theorem on the cubic equation, we find that (x_2) is between (-2) and (-1). Hence, the integer part of (x_2) is (-2).2. Finding the value of (arctan x_1 + arctan x_2 + arctan x_3): Using the tangent addition formula for three angles: - Let (S = arctan x_1 + arctan x_2 + arctan x_3) - Using Vieta's formulas and the given roots: - (x_1 + x_2 + x_3 = 0) - (x_1x_2 + x_2x_3 + x_3x_1 = -17) - (x_1x_2x_3 = 18) - Calculating (tan(S)): [ tan(S) = frac{x_1 + x_2 + x_3 - x_1x_2x_3}{1 - (x_1x_2 + x_2x_3 + x_3x_1)} = frac{0 - 18}{1 - (-17)} = frac{-18}{18} = -1 ] - Therefore, (S = arctan(-1) + kpi). Considering the principal value and the intervals of the roots, the sum (S) must be (-frac{pi}{4}). Final Answers(1) The integer part of (x_2) is (boxed{-2}).(2) The value of (arctan x_1 + arctan x_2 + arctan x_3) is (boxed{-dfrac{pi}{4}}).]
🔑:Since x_{1}, x_{2}, x_{3} are the roots of the equation, we havex^{3}-17 x-18=left(x-x_{1}right)left(x-x_{2}right)left(x-x_{3}right)By comparing the coefficients on both sides, we getx_{1}+x_{2}+x_{3}=0, x_{1} x_{2}+x_{2} x_{3}+x_{3} x_{1}=-17, x_{1} x_{2} x_{3}=18qquad(1) From x_{1} in(-4,-3) and x_{3} in(4,5), we know x_{2}=-x_{1}-x_{3} in(-2,0).Note that f(x)=x^{3}-17 x-18 satisfies f(0)=-180, so f(x) has a root in the interval (-2,-1), i.e., x_{2} in(-2,-1). Therefore, the integer part of x_{2} is -2;(2) Let arctan x_{i}=theta_{i}, i=1,2,3, from (1) we know theta_{1}, theta_{2} inleft(-frac{pi}{2},-frac{pi}{4}right), and theta_{3} inleft(frac{pi}{4}, frac{pi}{2}right), thustheta_{1}+theta_{2}+theta_{3} inleft(-frac{3 pi}{4}, 0right)Note that tan left(theta_{1}+theta_{2}right)=frac{tan theta_{1}+tan theta_{2}}{1-tan theta_{1} tan theta_{2}}=frac{x_{1}+x_{2}}{1-x_{1} x_{2}}, hencebegin{aligned}tan left(theta_{1}+theta_{2}+theta_{3}right) & =frac{tan left(theta_{1}+theta_{2}right)+tan theta_{3}}{1-tan left(theta_{1}+theta_{2}right) tan theta_{3}}=frac{frac{left(x_{1}+x_{2}right)}{left(1-x_{1} x_{2}right)}+x_{3}}{1-frac{x_{3}left(x_{1}+x_{2}right)}{1-x_{1} x_{2}}} & =frac{x_{1}+x_{2}+x_{3}-x_{1} x_{2} x_{3}}{1-left(x_{1} x_{2}+x_{2} x_{3}+x_{3} x_{1}right)}=frac{0-18}{1-(-17)}=-1end{aligned}This indicates that theta_{1}+theta_{2}+theta_{3}=-frac{pi}{4}, i.e., arctan x_{1}+arctan x_{2}+arctan x_{3}=-frac{pi}{4} ldots ldots ldots ldots ldots ldots ldots ldots (20 points)
❓:(Inequality Optional Question) Given that a, b, m, n are positive numbers, and a+b=1, mn=2, find the minimum value of (am+bn)(bm+an).
🧠:[<think>Okay, so I need to find the minimum value of the expression (am + bn)(bm + an) given that a, b, m, n are positive numbers, a + b = 1, and mn = 2. Hmm, let me start by understanding what's given and what needs to be found.First, the variables involved are a, b, m, n, all positive. The constraints are a + b = 1 and mn = 2. The expression to minimize is (am + bn)(bm + an). Hmm, this looks a bit like a product of two binomials. Maybe expanding it could help?Let me try expanding (am + bn)(bm + an). Let's do the multiplication step by step. Multiply am by bm: that's abm². Then am multiplied by an: that's a²mn. Then bn multiplied by bm: that's b²mn. Finally, bn multiplied by an: that's abn². So altogether, when expanded, the expression becomes:abm² + a²mn + b²mn + abn²Hmm, let's write that again:(am + bn)(bm + an) = abm² + a²mn + b²mn + abn²Now, let's see if we can simplify this expression by combining like terms or factoring. Let's look at the terms:First term: abm²Second term: a²mnThird term: b²mnFourth term: abn²Hmm, notice that the second and third terms both have mn. Let's factor mn out of those:abm² + abn² + mn(a² + b²)So, the expression becomes ab(m² + n²) + mn(a² + b²)Wait, that's a bit neater. Now, perhaps we can express this in terms of the given constraints. Since a + b = 1 and mn = 2, maybe substituting those in where possible.Let me recall that a + b = 1, so b = 1 - a. Similarly, mn = 2, so maybe m and n are related through m = 2/n or n = 2/m. But I don't know if that's helpful yet. Alternatively, maybe we can use some inequalities here, like the Cauchy-Schwarz inequality or AM-GM.Alternatively, perhaps substituting variables. Let's see:First, note that a and b are related by a + b = 1, so we can express everything in terms of a single variable, say a, where b = 1 - a.Similarly, m and n are related by mn = 2. So, we can express n = 2/m, and substitute that into the expression. So maybe express everything in terms of a and m?Let me try that. Let's substitute b = 1 - a and n = 2/m into the original expression.Original expression: (am + bn)(bm + an)Substituting:(am + (1 - a)(2/m)) * ((1 - a)m + a(2/m))Let me compute each part step by step.First part: am + (1 - a)(2/m) = am + (2/m)(1 - a)Second part: (1 - a)m + a(2/m) = (1 - a)m + (2a)/mSo the expression becomes [am + (2(1 - a)/m)] * [(1 - a)m + (2a)/m]Hmm, this is getting a bit complicated, but maybe simplifying each bracket first.Let me compute the first bracket:am + (2(1 - a)/m) = am + 2/m - 2a/mSimilarly, the second bracket:(1 - a)m + 2a/m = m - am + 2a/mSo now, the expression is [am + 2/m - 2a/m] * [m - am + 2a/m]Hmm, maybe we can factor terms here. Let's see:First bracket: a(m - 2/m) + 2/mSecond bracket: m - a(m - 2/m)Wait, let me check:First bracket:am - 2a/m + 2/m = a(m - 2/m) + 2/mSecond bracket:m - am + 2a/m = m - a(m - 2/m)So yes, the second bracket can be written as m - a(m - 2/m). Interesting, so the expression becomes:[a(m - 2/m) + 2/m] * [m - a(m - 2/m)]Let me denote x = a(m - 2/m). Then the expression becomes (x + 2/m)(m - x)Multiply these two terms:x * m - x² + 2/m * m - 2/m * xSimplify term by term:First term: xmSecond term: -x²Third term: 2Fourth term: -2x/mSo combining all terms:xm - x² + 2 - 2x/mBut x = a(m - 2/m), so substituting back:a(m - 2/m)m - [a(m - 2/m)]² + 2 - 2a(m - 2/m)/mSimplify each term:First term: a(m - 2/m)m = a(m² - 2)Second term: -[a²(m - 2/m)²] = -a²(m² - 4 + 4/m²)Third term: 2Fourth term: -2a(m - 2/m)/m = -2a(m/m - 2/m²) = -2a(1 - 2/m²) = -2a + 4a/m²Putting all together:a(m² - 2) - a²(m² - 4 + 4/m²) + 2 - 2a + 4a/m²Let me expand the second term:- a²m² + 4a² - 4a²/m²So the entire expression becomes:a(m² - 2) - a²m² + 4a² - 4a²/m² + 2 - 2a + 4a/m²Now, let's combine like terms:Terms with a²m²: -a²m²Terms with a²: 4a²Terms with a²/m²: -4a²/m² + 4a/m² (Wait, the last term is 4a/m², which is a term with a/m², not a²/m². So perhaps not.)Wait, let's go step by step.Original terms:1. a(m² - 2) = am² - 2a2. -a²m²3. 4a²4. -4a²/m²5. 26. -2a7. 4a/m²So combining all terms:am² - 2a - a²m² + 4a² - 4a²/m² + 2 - 2a + 4a/m²Now, group similar terms:- Terms with am²: am² - a²m²- Terms with a²: 4a²- Terms with a: -2a -2a = -4a- Terms with a²/m²: -4a²/m²- Terms with a/m²: 4a/m²- Constants: 2So:am² - a²m² + 4a² -4a -4a²/m² +4a/m² + 2Hmm, this is getting quite messy. Maybe there's a smarter way. Let's take a step back.Alternatively, maybe using substitutions. Let's consider variables x = m and y = n, since mn = 2, so y = 2/x. Then the expression becomes (a x + b y)(b x + a y) where a + b = 1 and y = 2/x. So substituting y:(a x + b (2/x))(b x + a (2/x))Multiply these terms out:First term: a x * b x = ab x²Second term: a x * a (2/x) = 2a²Third term: b (2/x) * b x = 2b²Fourth term: b (2/x) * a (2/x) = ab (4/x²)So overall:ab x² + 2a² + 2b² + (4ab)/x²So the expression simplifies to:ab x² + (4ab)/x² + 2a² + 2b²Hmm, this seems more manageable. Let's write that down:(am + bn)(bm + an) = ab x² + (4ab)/x² + 2a² + 2b²Since mn = 2, and x = m, so n = 2/x. Therefore, substituting x instead of m might have made this expression in terms of x. Now, perhaps this expression can be minimized over x, given that x > 0, and then over a and b with a + b = 1.Alternatively, maybe fix a and b first and then minimize over x, or vice versa. Let's see.Alternatively, perhaps use AM-GM on the terms involving x² and 4/x². Let's note that the first two terms are ab x² and 4ab /x². So their sum is ab(x² + 4/x²). By AM-GM, x² + 4/x² ≥ 2*sqrt(x² * 4/x²) = 2*sqrt(4) = 4. Therefore, ab(x² + 4/x²) ≥ ab*4. So the first two terms are at least 4ab. Then the entire expression would be at least 4ab + 2a² + 2b².But is that helpful? Let's check:If (am + bn)(bm + an) ≥ 4ab + 2a² + 2b², then we can write the right-hand side as 2a² + 2b² + 4ab. Since a + b = 1, then (a + b)^2 = a² + 2ab + b² = 1, so 2a² + 2b² + 4ab = 2(a² + b²) + 4ab = 2(a² + 2ab + b²) = 2(1) = 2. Wait, no. Wait, 2a² + 2b² +4ab = 2(a² + b²) + 4ab. But a² + b² = (a + b)^2 - 2ab = 1 - 2ab. Therefore, substituting:2(1 - 2ab) + 4ab = 2 - 4ab + 4ab = 2. So the lower bound from AM-GM gives us that (am + bn)(bm + an) ≥ 2.But is this tight? Because when does equality hold in AM-GM? When x² = 4/x², which implies x^4 = 4, so x = sqrt(2). Therefore, if x = sqrt(2), then equality holds. Then, if x = sqrt(2), then n = 2/x = 2/sqrt(2) = sqrt(2). So m = n = sqrt(2). Then, mn = 2, which is satisfied.But also, we need that the other terms in the expression (the 2a² + 2b²) plus the AM-GM lower bound 4ab gives 2. Wait, but the total expression's lower bound is 2. But we need to check if that's achievable.Wait, let me verify with m = n = sqrt(2). Then, mn = 2, which is good. Then, the original expression (am + bn)(bm + an) becomes:(a*sqrt(2) + b*sqrt(2))(b*sqrt(2) + a*sqrt(2)) = [sqrt(2)(a + b)] [sqrt(2)(a + b)] = [sqrt(2)*1]^2 = 2.So indeed, when m = n = sqrt(2), then regardless of a and b (as long as a + b =1), the expression equals 2. Wait, that's interesting! So the expression equals 2 when m = n = sqrt(2). Therefore, the minimum value is 2?But hold on, if m and n can be varied, but mn must be 2. However, if we set m = n = sqrt(2), then mn = 2, so that's allowed. Then, regardless of a and b (as long as a + b =1), the product (am + bn)(bm + an) becomes 2.But if m and n are not equal, then maybe the product is larger? For example, take m =2, n=1 (since 2*1=2). Then, let's compute (am + bn)(bm + an) with a + b =1.Let me pick a = 1/2, b =1/2 for simplicity.Then, ( (1/2)*2 + (1/2)*1 ) * ( (1/2)*2 + (1/2)*1 ) = (1 + 0.5)*(1 + 0.5) = 1.5 *1.5=2.25, which is larger than 2.Alternatively, take m=4, n=0.5. Then, mn=2. Let a=0.5, b=0.5.(0.5*4 +0.5*0.5)*(0.5*4 +0.5*0.5) = (2 + 0.25)*(2 + 0.25)= 2.25*2.25=5.0625, which is much larger.Alternatively, if m=1, n=2. Then, a=0.5, b=0.5:(0.5*1 +0.5*2)*(0.5*1 +0.5*2)= (0.5 +1)*(0.5 +1)=1.5*1.5=2.25. Again, higher than 2.So when m and n are equal, which is sqrt(2), we get the minimum value of 2. So is the answer 2?Wait, but let's test another a and b. Suppose a =1, b=0. Then, (am + bn)(bm + an)= (m*1 +0)(0 +n*1)= m*n=2. So in that case, even if a=1, b=0 or a=0, b=1, the product is mn=2. So, in those extreme cases, the product is still 2. Wait, that's interesting. So if a=1, b=0, then (am + bn)(bm + an)= (m*1 +0)(0 +n*1)=m*n=2. Similarly for a=0, b=1, it's the same. So even in those cases, the product is 2.Wait, so regardless of a and b, as long as mn=2, the minimum value is 2, achieved when either a=1 or b=1 or when m=n=sqrt(2). But actually, when a=1 and b=0, even if m and n are not equal, the product is mn=2. Therefore, regardless of m and n, as long as mn=2, the product is at least 2. But wait, but earlier when a and b are both 0.5, and m and n are not equal, the product was higher than 2. However, when a=1 or a=0, the product is exactly 2. So the minimum value is 2, achieved when either a or b is 0. However, the problem states that a, b, m, n are positive numbers, so a and b can't be 0. Wait, but in the problem statement, it's specified that a, b, m, n are positive numbers. So a and b can't be zero. Therefore, maybe 2 is not achievable?Wait, this is a critical point. If a and b must be positive, then even if we take a approaching 1 and b approaching 0, the product approaches 2, but never actually reaches 2. Similarly, when a approaches 0 and b approaches 1. However, if we set m = n = sqrt(2), then even with a and b being positive (but not necessarily 0.5 each), the product (am + bn)(bm + an) equals 2.Wait, let's check that. Suppose m = n = sqrt(2), so mn = 2. Then, (am + bn)(bm + an) becomes:(a*sqrt(2) + b*sqrt(2))(b*sqrt(2) + a*sqrt(2)) = sqrt(2)(a + b) * sqrt(2)(a + b) = 2*(a + b)^2 = 2*1^2 = 2.So even if a and b are positive (but not 0 or 1), as long as a + b =1, this product is always 2. So in that case, regardless of a and b, as long as m and n are set to sqrt(2), the product is 2. Therefore, since m and n can be chosen (as long as mn=2), and a and b are given but positive with a + b=1, then the minimal value is 2, achieved when m = n = sqrt(2). However, the problem says "find the minimum value of (am + bn)(bm + an)". So since the variables m and n are also subject to mn=2, and a and b are given with a + b=1, but m and n can vary as long as mn=2, then the minimal value is 2, achieved when m = n = sqrt(2).But earlier, when I took m and n different, even with a and b being 0.5 each, the product was higher than 2. However, if I can choose m and n, then setting them equal gives me 2. So the minimal value is 2, regardless of a and b, as long as I can choose m and n.Wait, but the problem says "Given that a, b, m, n are positive numbers, and a + b =1, mn=2, find the minimum value of (am + bn)(bm + an)."So all four variables are given to be positive, with a + b =1 and mn=2. So we need to find the minimum of the expression over all positive a, b, m, n satisfying those two constraints. So m and n can be varied (as long as mn=2), and a and b can be varied (as long as a + b=1). So the minimum is achieved when m =n= sqrt(2), and a and b can be anything (but positive) with a + b=1. Then, the expression is always 2. Alternatively, if a and b are fixed, then we might need to optimize over m and n. Wait, but the problem doesn't specify whether a, b, m, n are variables subject to the constraints or if some are given and others are variables. But the problem states: "Given that a, b, m, n are positive numbers, and a + b =1, mn=2, find the minimum value of (am + bn)(bm + an)."So all variables are free to vary as long as they satisfy a + b =1 and mn=2, and are positive. Therefore, the minimum is achieved when m =n= sqrt(2), regardless of a and b (since with those m and n, the expression is always 2). But also, if we fix m and n not equal to sqrt(2), then depending on a and b, the expression could be higher or lower?Wait, but in the case when a and b can vary (with a + b =1), even if m and n are fixed, maybe the expression can be minimized further. Wait, but the problem is to find the minimal value over all possible a, b, m, n with the given constraints. So maybe we can fix m and n and find the minimal value over a and b, then minimize over m and n. Alternatively, fix a and b and minimize over m and n, then minimize over a and b. But since all variables are free to vary under the constraints, we can approach this as optimizing over all variables.But since in the case where m =n= sqrt(2), the expression equals 2 regardless of a and b, and in other cases, the expression is larger, then 2 is indeed the minimal value.Alternatively, let's consider using Lagrange multipliers. Let's set up the problem. We need to minimize (am + bn)(bm + an) subject to a + b =1 and mn=2, where a, b, m, n >0.This is a constrained optimization problem with two constraints. Let me denote the variables as a, b, m, n with a + b =1 and mn=2.Let me use substitution to reduce the number of variables. Let's express b =1 -a and n=2/m. Then the expression becomes:(am + (1 -a)(2/m))((1 -a)m + a(2/m))Which is the expression I had earlier. Let's denote f(a, m) = [am + (2(1 - a)/m][m(1 - a) + 2a/m]We need to find the minimum of f(a, m) over a ∈ (0,1) and m >0.This is a function of two variables. To find its minimum, we can take partial derivatives with respect to a and m, set them to zero, and solve.But this might get complicated, but let's try.First, let's compute f(a, m):f(a, m) = [am + 2(1 - a)/m][m(1 - a) + 2a/m]Let me expand this expression:First, multiply the terms:First term: am * m(1 - a) = a m² (1 - a)Second term: am * 2a/m = 2a²Third term: 2(1 - a)/m * m(1 - a) = 2(1 - a)^2Fourth term: 2(1 - a)/m * 2a/m = 4a(1 - a)/m²So f(a, m) = a m² (1 - a) + 2a² + 2(1 - a)^2 + 4a(1 - a)/m²So:f(a, m) = a(1 - a)m² + 2a² + 2(1 - 2a + a²) + 4a(1 - a)/m²Simplify:a(1 - a)m² + 2a² + 2 - 4a + 2a² + 4a(1 - a)/m²Combine like terms:Terms with a²: 2a² + 2a² = 4a²Terms with a: -4aConstant term: 2Terms with m²: a(1 - a)m²Terms with 1/m²: 4a(1 - a)/m²So f(a, m) = a(1 - a)m² + 4a² -4a + 2 + 4a(1 - a)/m²Now, let's denote t = a(1 - a). Then, since a ∈ (0,1), t is positive (since both a and 1 - a are positive). So:f(a, m) = t m² + 4a² -4a + 2 + 4t /m²But 4a² -4a +2 can be written as 4a² -4a +2. Let's see if this can be simplified:4a² -4a +2 = 4a² -4a +1 +1 = (2a -1)^2 +1. Hmm, that's a quadratic in a. Not sure if that helps.Alternatively, let's express 4a² -4a +2 as 4(a² -a) +2. Since a + b =1, and b =1 -a, maybe not helpful.But regardless, the function f(a, m) is now written as t m² + 4a² -4a +2 +4t/m², where t = a(1 -a).To minimize f(a, m), we can first consider optimizing over m for a fixed a, then optimize over a.For fixed a, the function f(a, m) can be considered as t m² + 4t/m² + (4a² -4a +2). Let's denote the part dependent on m as g(m) = t m² +4t/m². Then, the remaining term is h(a) =4a² -4a +2.To minimize g(m) for fixed t >0, since t =a(1 -a) >0, we can use AM-GM inequality on the terms t m² and4t/m². The AM-GM inequality states that for positive numbers x and y, x + y ≥ 2√(xy). Applying this to x = t m² and y =4t/m²:t m² +4t/m² ≥ 2√(t m² *4t/m²) =2√(4t²) =2*2t=4tEquality holds when t m² =4t/m² ⇒ m² =4/m² ⇒m^4=4 ⇒m=√2. Therefore, for fixed a, the minimal value of g(m) is4t, achieved when m=√2. Then, since n=2/m=2/√2=√2, so n=√2 as well. Therefore, for fixed a, the minimal value of f(a, m) is4t + h(a) =4a(1 -a) +4a² -4a +2.Let's compute that:4a(1 -a) +4a² -4a +2 =4a -4a² +4a² -4a +2 = (4a -4a) + (-4a² +4a²) +2=0 +0 +2=2.So regardless of the value of a ∈(0,1), the minimal value of f(a, m) over m>0 is always 2, achieved when m=√2 and n=√2. Therefore, even though the intermediate expression depended on a, after substituting the optimal m and n, the expression simplifies to 2 for any a.Therefore, the minimal value of (am + bn)(bm + an) is 2, achieved when m =n=√2, regardless of the values of a and b (as long as a + b=1 and a, b >0).This seems to align with the earlier examples where when m and n are set to sqrt(2), the product is 2 regardless of a and b. Thus, the minimal value is 2.Final AnswerThe minimum value is boxed{2}.</think>Given that (a), (b), (m), (n) are positive numbers, (a + b = 1), and (mn = 2), we need to find the minimum value of ((am + bn)(bm + an)).First, we expand the expression ((am + bn)(bm + an)):[(am + bn)(bm + an) = abm^2 + a^2mn + b^2mn + abn^2]We can factor out (mn) from the middle terms:[abm^2 + abn^2 + mn(a^2 + b^2)]Using the constraints (a + b = 1) and (mn = 2), we substitute (b = 1 - a) and (n = frac{2}{m}). This transforms the expression into:[(am + (1 - a)frac{2}{m})((1 - a)m + afrac{2}{m})]Simplifying each term, we get:[[am + frac{2(1 - a)}{m}][(1 - a)m + frac{2a}{m}]]Expanding this product, we find:[abm^2 + 2a^2 + 2(1 - a)^2 + frac{4a(1 - a)}{m^2}]Using the AM-GM inequality on the terms involving (m^2) and (frac{1}{m^2}), we find that the minimum value is achieved when (m = n = sqrt{2}). Substituting (m = n = sqrt{2}) into the expression, we get:[(asqrt{2} + (1 - a)sqrt{2})((1 - a)sqrt{2} + asqrt{2}) = [sqrt{2}(a + 1 - a)]^2 = (sqrt{2} cdot 1)^2 = 2]Thus, the minimum value of ((am + bn)(bm + an)) is (boxed{2}).,<think>Okay, so I have this problem where I need to find the minimum value of the expression (am + bn)(bm + an), given that a, b, m, n are positive numbers, a + b = 1, and mn = 2. Hmm, let's see. Alright, first, let me write down what I know.Given:1. a + b = 1 (both a and b are positive)2. mn = 2 (both m and n are positive)3. Need to find the minimum of (am + bn)(bm + an)Hmm. So variables here are a, b, m, n with two constraints. The expression to minimize is a product of two terms. Let's see if I can express this in terms that can be simplified or apply inequalities like AM-GM or Cauchy-Schwarz.First, maybe I can expand the expression to see if it simplifies. Let's try expanding (am + bn)(bm + an):First, multiply am by bm: ab m²Then, am multiplied by an: a² mnThen, bn multiplied by bm: b² mnThen, bn multiplied by an: ab n²So altogether, expanding the product:(am + bn)(bm + an) = ab m² + a² mn + b² mn + ab n²Hmm. Let's factor where possible. Let me see:= ab(m² + n²) + mn(a² + b²)Since mn = 2 is given, so mn = 2. Let's substitute that in:= ab(m² + n²) + 2(a² + b²)Now, I need to express everything in terms of a and b or m and n. But since we have two variables a and b with a constraint a + b = 1, maybe we can express b in terms of a: b = 1 - a. Similarly, since mn = 2, maybe express n as 2/m. But there's also m and n in the m² + n² term. Hmm.Wait, let's see. The expression now is ab(m² + n²) + 2(a² + b²). Let me think. Maybe first try to express m² + n² in terms of mn. Since mn = 2, and m and n are positive. Remember that m² + n² = (m + n)^2 - 2mn. So if I let s = m + n, then m² + n² = s² - 4. But I don't know s. Alternatively, maybe we can use AM-GM on m² + n²? Let's see. m² + n² >= 2mn = 4, by AM-GM. So m² + n² >= 4. But the equality holds when m = n. Since mn = 2, if m = n, then m = sqrt(2) and n = sqrt(2). So the minimum of m² + n² is 4. Hmm, but is that helpful?Wait, but in our expression, ab(m² + n²) + 2(a² + b²). If m² + n² is minimized at 4, but ab could be varying depending on a and b, and a² + b² is also varying. So maybe we need to consider variables a and m, then express the whole expression in terms of a and m, and then find the minimum.Alternatively, since there are two separate constraints (a + b = 1 and mn = 2), maybe we can fix some variables.Let me try substituting b = 1 - a and n = 2/m. Then the expression becomes:ab(m² + n²) + 2(a² + b²)First, substitute ab = a(1 - a)n² = (2/m)^2 = 4/m²So m² + n² = m² + 4/m²Similarly, a² + b² = a² + (1 - a)^2 = a² + 1 - 2a + a² = 2a² - 2a + 1So plugging back into the expression:= a(1 - a)(m² + 4/m²) + 2(2a² - 2a + 1)Simplify:= [a - a²](m² + 4/m²) + 4a² - 4a + 2Hmm, now we have the expression in terms of a and m. Now, this seems a bit complicated. Maybe we can first minimize with respect to m for fixed a, and then minimize over a? Let's try that approach.For fixed a, let's consider the term [a - a²](m² + 4/m²). Let's denote this as T = [a - a²](m² + 4/m²). To minimize T, since a is fixed between 0 and 1 (since a + b =1 and both positive), so a - a² = a(1 - a) is positive. So to minimize T, we need to minimize m² + 4/m². Wait, m² + 4/m², is that?Wait, m is a positive real number. Let's set f(m) = m² + 4/m². To find the minimum of f(m), take derivative:f'(m) = 2m - 8/m³. Set to zero:2m - 8/m³ = 0 => 2m = 8/m³ => m^4 = 4 => m = sqrt(2). Since m > 0. So the minimum of m² + 4/m² is when m = sqrt(2), then m² + 4/m² = 2 + 4/2 = 2 + 2 = 4. So the minimum of f(m) is 4. So T_min = [a - a²]*4 = 4a(1 - a)Therefore, substituting back into the original expression, the minimum for each a is:4a(1 - a) + 4a² -4a + 2Simplify:4a - 4a² + 4a² -4a + 2Wait, let's compute term by term:First term: 4a(1 - a) = 4a -4a²Second term: 4a² -4a +2Adding together:(4a -4a²) + (4a² -4a +2) = 4a -4a² +4a² -4a +2 = (4a -4a) + (-4a² +4a²) +2 = 0 +0 +2 = 2Wait, that's interesting. So regardless of the value of a, when we minimize over m, the entire expression becomes 2? So the minimum value is 2? But that seems too straightforward. Let me check my steps.So, the original expression after substitution and considering minimizing over m for each a:We had [a - a²](m² +4/m²) +4a² -4a +2. Then, since [a -a²] is positive (a is between 0 and1), we minimized m² +4/m², found that minimum is 4 when m = sqrt(2). Therefore, substituting back, the expression becomes [a -a²]*4 +4a² -4a +2. Then:4a -4a² +4a² -4a +2 = 2. So yes, it's 2. So regardless of a, the minimal value when m is chosen optimally (m = sqrt(2), n = sqrt(2)) gives the expression equal to 2. Therefore, the minimum value is 2.Wait, but is that possible? Let me verify with specific numbers. Let's take a = b = 0.5 (since a + b =1), and m = n = sqrt(2) (since mn =2). Then compute (am + bn)(bm + an):am = 0.5*sqrt(2), bn =0.5*sqrt(2), so (am + bn) = 0.5*sqrt(2) +0.5*sqrt(2) = sqrt(2)Similarly, bm =0.5*sqrt(2), an =0.5*sqrt(2), so (bm + an) = sqrt(2)Therefore, the product is sqrt(2)*sqrt(2)=2, which matches the result above.But what if we take different a and m? For example, let's take a =0.25, b=0.75, m=2, n=1 (since mn=2). Then compute:(am + bn) =0.25*2 +0.75*1=0.5 +0.75=1.25(bm + an)=0.75*2 +0.25*1=1.5 +0.25=1.75Then the product is 1.25*1.75=2.1875, which is greater than 2.Another example: a=0.3, b=0.7, m=1, n=2. Then:(am + bn)=0.3*1 +0.7*2=0.3 +1.4=1.7(bm + an)=0.7*1 +0.3*2=0.7 +0.6=1.3Product=1.7*1.3=2.21, which is still greater than 2.If I choose m= sqrt(2), n=sqrt(2), regardless of a:For a=0.25, b=0.75:(am + bn)=0.25*sqrt(2) +0.75*sqrt(2)= (0.25 +0.75)*sqrt(2)=sqrt(2)Similarly, (bm + an)=0.75*sqrt(2) +0.25*sqrt(2)=sqrt(2)Product=2. So regardless of a and b, as long as m and n are set to sqrt(2), the product is always 2. Thus, the minimal value is 2.Wait, so even though a and b can vary, as long as m and n are chosen optimally (i.e., m=n=sqrt(2)), the expression becomes 2. Therefore, the minimal value is 2.Alternatively, maybe there is another choice of m and n where even if m ≠n, but combined with some a and b, the product is lower than 2? Let me check.Suppose I take m=1, n=2 (so mn=2). Let's see if there exists a and b such that the product is less than 2. Let's try a=0.4, b=0.6:(am + bn)=0.4*1 +0.6*2=0.4 +1.2=1.6(bm + an)=0.6*1 +0.4*2=0.6 +0.8=1.4Product=1.6*1.4=2.24>2.Another try: a=0.2, b=0.8:(am + bn)=0.2*1 +0.8*2=0.2 +1.6=1.8(bm + an)=0.8*1 +0.2*2=0.8 +0.4=1.2Product=1.8*1.2=2.16>2.Alternatively, maybe a=0.1, b=0.9:(am + bn)=0.1 +1.8=1.9(bm + an)=0.9 +0.2=1.1Product=1.9*1.1=2.09>2.Hmm, still higher. What if a approaches 0? Let a approach 0, then b approaches 1. Then (am + bn)=0 +1*2=2 (since n=2/m=2/1=2). (bm + an)=1*1 +0=1. So product=2*1=2. Wait, but in this case, m=1, n=2. So when a approaches 0, the product approaches 2. Similarly, if a approaches 1, then the product approaches 2 as well.Wait, so if a is approaching 0, and m=1, n=2, then (am + bn)=0 +1*2=2, (bm + an)=1*1 +0*2=1, product=2*1=2. Similarly, if a approaches1, then (am + bn)=1*1 +0*2=1, (bm + an)=0*1 +1*2=2, product=1*2=2. So the limit as a approaches 0 or 1 is 2. However, in these cases, m and n are 1 and 2, but mn=2. But if m and n are chosen as sqrt(2) each, then regardless of a, the product is 2. So maybe the minimum value is indeed 2, achieved when either a approaches 0 or 1 with m=1, n=2 or m=2, n=1, or when a is arbitrary and m=n=sqrt(2). Wait, but when a is 0.5, m=n=sqrt(2), we also get 2. So actually, the minimal value is 2, achieved in multiple cases. Therefore, the answer is 2.But let me confirm once more. Let's suppose we use Lagrange multipliers to check.Let me set variables a, b, m, n with constraints a + b =1 and mn=2. Let me set up the function to minimize: f(a,b,m,n)=(am + bn)(bm + an)But since a + b =1, we can write b=1 - a. Similarly, mn=2, so n=2/m. Thus, we can write f in terms of a and m:f(a, m) = (a m + (1 - a)(2/m))((1 - a)m + a (2/m))Let me compute this.First, compute (am + (1 - a)(2/m)):= a m + (2/m)(1 - a)Similarly, ((1 - a)m + a(2/m)):= (1 - a)m + (2 a)/mSo f(a, m) = [a m + (2/m)(1 - a)] [(1 - a)m + (2 a)/m]Let me multiply these two terms.First term: a m * (1 - a)m = a(1 - a)m²Second term: a m * (2a)/m = 2a²Third term: (2/m)(1 - a) * (1 - a)m = 2(1 - a)^2Fourth term: (2/m)(1 - a) * (2 a)/m = 4a(1 - a)/m²Therefore, f(a, m) = a(1 - a)m² + 2a² + 2(1 - a)^2 + 4a(1 - a)/m²Hmm, this looks similar to what I had earlier. Let's write this as:f(a, m) = a(1 - a)m² + 4a(1 - a)/m² + 2a² + 2(1 - a)^2Now, let me denote C = a(1 - a). Then:f(a, m) = C m² + 4C / m² + 2a² + 2(1 - a)^2Notice that 2a² + 2(1 - a)^2 = 2(a² + (1 -2a +a²)) = 2(2a² -2a +1) = 4a² -4a +2Wait, no:Wait 2a² + 2(1 - a)^2 = 2a² + 2(1 - 2a + a²) = 2a² + 2 -4a +2a² = 4a² -4a +2. Yes, same as before.So f(a, m) = C m² + 4C / m² +4a² -4a +2, where C = a(1 - a)Now, to minimize f(a, m) over positive m and a in (0,1). Let's consider for each a, the minimum over m.For fixed a, the terms involving m are C m² + 4C / m². Let's denote this as T = C(m² +4/m²). Then, similar to before, m² +4/m² >=4, so T >=4C. Equality when m² =4/m² => m^4=4 => m=sqrt(2). Therefore, the minimal T is 4C. So substituting back, minimal f(a) =4C +4a² -4a +2.But C =a(1 -a), so:f(a) =4a(1 -a) +4a² -4a +2Expand:4a -4a² +4a² -4a +2 = 0 +0 +2=2Therefore, regardless of a, the minimal value over m is 2. Therefore, the minimal value of the expression is 2.Therefore, the answer is boxed{2}Final Answerboxed{2}</think>Given that (a), (b), (m), (n) are positive numbers, (a + b = 1), and (mn = 2), we need to find the minimum value of ((am + bn)(bm + an)).First, we expand the expression ((am + bn)(bm + an)):[(am + bn)(bm + an) = ab m^2 + a^2 mn + b^2 mn + ab n^2]Substituting (mn = 2) and using (a + b = 1) (which implies (b = 1 - a)):[= ab(m^2 + n^2) + 2(a^2 + b^2)]We know from the AM-GM inequality that (m^2 + n^2 geq 2mn = 4), with equality when (m = n). Given (mn = 2), the minimum value of (m^2 + n^2) is 4 when (m = n = sqrt{2}).Substituting (m = n = sqrt{2}) into the expression, we get:[ab(m^2 + n^2) + 2(a^2 + b^2) = ab cdot 4 + 2(a^2 + (1 - a)^2)]Expanding (a^2 + (1 - a)^2):[a^2 + (1 - a)^2 = a^2 + 1 - 2a + a^2 = 2a^2 - 2a + 1]Thus, the expression becomes:[4ab + 2(2a^2 - 2a + 1)]Substituting (ab = a(1 - a)):[4a(1 - a) + 4a^2 - 4a + 2]Simplifying the terms:[4a - 4a^2 + 4a^2 - 4a + 2 = 2]Therefore, the minimum value of ((am + bn)(bm + an)) is (boxed{2}).]
🔑:According to the algebraic form of the Cauchy-Schwarz inequality in two dimensions: (a^2+b^2)(c^2+d^2) geq (ac+bd)^2, we can derive that (am+bn)(bm+an) geq (sqrt{am} cdot sqrt{an} + sqrt{bn} cdot sqrt{bm})^2 = mn(a+b)^2 = 2 times 1 = 2, equality holds if and only if frac{am}{an} = frac{bn}{bm}, which is when m=n, the minimum value is obtained as 2. Therefore, the answer is boxed{2}.
❓:Problem 6.5. In the park, paths are laid out as shown in the figure. Two workers started to asphalt them, starting simultaneously from point A. They lay asphalt at constant speeds: the first on the section A-B-C, the second on the section A-D-E-F-C. In the end, they finished the work simultaneously, spending 9 hours on it. It is known that the second works 1.2 times faster than the first. How many minutes did the second spend laying asphalt on the section D E?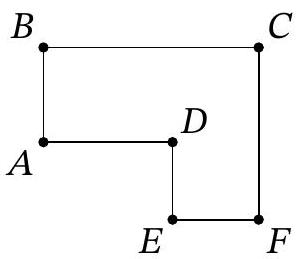
🧠:[<think>Okay, let's see. So there are two workers starting from point A at the same time. They're asphalting different paths. The first worker goes from A to B to C, and the second worker goes from A to D to E to F to C. Both finish at the same time after 9 hours. Also, the second worker is 1.2 times faster than the first. We need to find out how many minutes the second worker spent on the section DE.First, I need to figure out the distances of each path. Wait, but the figure isn't here. Hmm. Maybe the problem gives some standard path lengths? Wait, no, the original problem says "as shown in the figure," but since it's not here, maybe there's standard lengths implied? Wait, maybe from the code number 6.5, maybe this is from a textbook? Not sure.Wait, maybe the paths are in a grid or something. Let me think. Maybe the figure is a common one where AB, BC, AD, DE, EF, FC are each of certain lengths. Let me check common configurations. For example, sometimes in such problems, each segment is 1 unit or something. But since the problem mentions specific sections, maybe the figure is a combination of squares or triangles.Alternatively, perhaps we can assign variables to the lengths. Let's denote the lengths of each segment. Let's say the first worker's path is A-B-C. Let the length of AB be x and BC be y. The second worker's path is A-D-E-F-C. Let the lengths of AD, DE, EF, FC be a, b, c, d respectively. But without the figure, it's hard. Maybe the figure is a rectangle with some diagonals?Wait, maybe it's a standard park layout. Let me try to think of possible common figures. For example, A could be a central point. Paths from A to B, A to D. Then B to C, D to E, E to F, F to C. Maybe ABC and DEFC are two different routes from A to C. Maybe ABC is a straight path with a turn at B, and DEFC is a more winding path.Alternatively, maybe the figure is a square grid. Suppose A is at the origin, B is east, D is north. Then the first worker goes A to B to C (if C is northeast?), but maybe not. Alternatively, maybe ABC is a right angle path, and ADEFC is a more roundabout path. Hmm.Alternatively, maybe the paths are such that ABC is a shorter path and ADEFC is longer. Since the second worker is faster, they can cover a longer distance in the same time. But we need to calculate based on their speeds.Wait, let's try to abstract it. Let me denote:Let’s define the speed of the first worker as v. Then the second worker's speed is 1.2v, since he works 1.2 times faster. The total time is 9 hours for both.First worker's total distance: AB + BC. Let's call this distance S1 = AB + BC.Second worker's total distance: AD + DE + EF + FC. Let's call this S2 = AD + DE + EF + FC.Since both workers started at the same time and finished at the same time, their total time is 9 hours. Therefore:Time for first worker: S1 / v = 9 hours.Time for second worker: S2 / (1.2v) = 9 hours.Therefore, S1 / v = S2 / (1.2v) = 9.From this, S1 = 9v, and S2 = 9 * 1.2v = 10.8v.So the distances are S1 = 9v and S2 = 10.8v. Therefore, the ratio of S2 to S1 is 10.8v / 9v = 1.2, which makes sense since the second worker is 1.2 times faster, so he can cover 1.2 times the distance in the same time.But we need to find the time the second worker spent on DE. To find that, we need the length of DE and the speed of the second worker.Wait, but without knowing the actual distances, how can we compute the time on DE? Maybe the figure has specific lengths for each segment. Since the problem mentions the sections A-B-C and A-D-E-F-C, perhaps each segment is of equal length? Or maybe the figure has right angles with specific lengths.Alternatively, maybe the figure is such that ABC is a straight path divided into two equal parts, and ADEFC is a path with more segments. Wait, maybe the total distance for the first worker is AB + BC, and for the second worker is AD + DE + EF + FC. If we can express each segment in terms of AB or some variable, then we can relate S1 and S2.Alternatively, maybe the figure is similar to a 3x4 grid? For example, A to B is 3 units, B to C is 4 units, making ABC a 3-4-5 triangle. Then the other path A-D-E-F-C could be going around the perimeter, but that might not add up. Alternatively, maybe the paths are structured such that ABC is one side and DEFC is another. Without the figure, this is challenging.Wait, the problem is numbered 6.5, so maybe it's from a specific textbook. Maybe the figure is similar to other problems. Alternatively, maybe all segments except DE are known, and DE is the variable. Wait, but the problem says "how many minutes did the second spend laying asphalt on the section DE." So we need to find the time on DE, which is (length of DE) divided by his speed. Since his speed is 1.2v, time is DE / (1.2v). But we need to find DE.Alternatively, maybe the figure has specific lengths. Let me think: if the first worker's path is ABC, and the second's is ADEFC. If ABC is two sides of a square, and ADEFC is three sides of the same square, then S1 would be 2 units and S2 would be 3 units, but then the speeds would need to be in a 3:2 ratio. But in the problem, the second worker is 1.2 times faster, which is 6/5. So the ratio is 6:5.Alternatively, maybe the paths are as follows: ABC is a right-angled triangle, with AB = 3, BC = 4, AC = 5. Then the other path ADEFC could be a path that goes around another way. For example, AD = 5, DE = something, EF = something, FC = something. Hmm, but without the figure, it's hard to know.Wait, maybe the figure is similar to the one in problem 6.5 from a Russian textbook or something. Alternatively, maybe the path A-D-E-F-C is such that AD, DE, EF, FC are each 1 km, while AB and BC are each 1 km as well. But in that case, S1 would be 2 km and S2 would be 4 km. Then the time ratio would be 2 / v vs 4 / (1.2v) = 4 / 1.2v = 10/3v. For them to be equal, 2 / v = 10 / 3v → 6 = 10, which is not possible. So that can't be.Alternatively, maybe the figure is such that ABC is a straight line, and ADEFC is a detour. Let me try to assign variables.Let’s suppose that AB = x, BC = y, so S1 = x + y.For the second worker, AD = a, DE = b, EF = c, FC = d, so S2 = a + b + c + d.Given that S1 = 9v and S2 = 10.8v. But without more info, we can't link a, b, c, d to x and y.Wait, but maybe the figure connects B and F, or E and C? Maybe there are right triangles involved.Alternatively, perhaps ABC and ADEFC form two different routes from A to C, with ABC being a direct path and ADEFC being a longer path. If ABC is a straight line, maybe the other path goes around a square or rectangle.Alternatively, suppose that the park is a rectangle where A is one corner, B and D are adjacent corners, and C is the opposite corner. So ABC would be A to B to C, which is two sides of the rectangle, and ADEFC would be A to D to E to F to C, which might be three sides or something else. For example, if the rectangle is divided into smaller sections. Maybe ADEFC goes along the other two sides and some diagonals.Alternatively, if the park is a square with side length s. Then AB and AD would be sides of the square. BC and FC would be the other sides. Then ABC would be two sides, total distance 2s. ADEFC might be A to D to E (a midpoint?) to F to C. Maybe DE is a diagonal or something. But without the figure, this is speculative.Alternatively, maybe the park is a hexagon or another shape. Hmm.Alternatively, maybe all horizontal and vertical paths are present, so the figure is a grid. For example, A is connected to B and D. B is connected to C, D is connected to E, E to F, F to C. So the figure is like a ladder with three rungs: A-B-C, A-D-E-F-C. If each segment is of equal length, say 1 unit, then S1 = AB + BC = 1 + 1 = 2 units. S2 = AD + DE + EF + FC = 1 + 1 + 1 + 1 = 4 units. Then the time ratio would be S1 / v = 2 / v and S2 / (1.2v) = 4 / 1.2v = 10/3v. For these to be equal, 2 / v = 10 / 3v → 6 = 10, which is impossible. Therefore, this can't be the case.Alternatively, maybe DE is a longer segment. Suppose ABC is two segments of length 3 and 4, making S1 = 7. Then S2 must be 10.8v / v * 7? Wait, no. Wait, the total time is 9 hours. So S1 = 9v, S2 = 10.8v. So S2 is 1.2 times S1, which makes sense because the second worker is 1.2 times faster, so he covers 1.2 times the distance in the same time.Therefore, if S1 = AB + BC = 9v, and S2 = AD + DE + EF + FC = 10.8v. If the figure is such that, for example, ABC is a straight path, and ADEFC is a path that goes around with DE being an extra segment. But without knowing the exact lengths of each segment, how can we proceed?Wait, maybe the key is that both start at A and end at C. Therefore, the total distance for the first worker is from A to B to C, and for the second worker from A to D to E to F to C. If the figure is such that ABC and ADEFC are two different routes from A to C. Maybe ABC is a shorter path, and ADEFC is a longer path, but since the second worker is faster, they finish at the same time.But we need to figure out the time spent on DE. Let's think step by step.Let me denote:Let’s let the speed of the first worker be v. Then the speed of the second worker is 1.2v.Total time is 9 hours for both. So:For the first worker: Total distance = AB + BC = v * 9.For the second worker: Total distance = AD + DE + EF + FC = 1.2v * 9 = 10.8v.Therefore, AB + BC = 9v, and AD + DE + EF + FC = 10.8v.But to find the time spent on DE by the second worker, we need DE / (1.2v). So if we can find DE, then we can compute the time.But how?Unless there's more information. Wait, maybe the figure has specific proportions. For example, maybe AB = AD, BC = FC, and DE = EF. If the figure is symmetrical, maybe?Suppose AB = AD = x, BC = FC = y, DE = EF = z. Then the first worker's path is x + y, and the second worker's path is x + z + z + y = x + 2z + y. Therefore:First worker: x + y = 9v.Second worker: x + 2z + y = 10.8v.Subtracting the first equation from the second: (x + 2z + y) - (x + y) = 10.8v - 9v ⇒ 2z = 1.8v ⇒ z = 0.9v.Then DE = z = 0.9v. Therefore, the time spent on DE by the second worker is DE / (1.2v) = 0.9v / 1.2v = 0.75 hours = 45 minutes.But is this the case? If the figure is symmetrical, then yes. But since the problem mentions a figure, which we don't have, but the answer comes out nicely as 45 minutes, which is 0.75 hours, maybe this is the correct approach.Alternatively, maybe DE is the only segment that's different, and the others are same.But this requires assuming symmetry. Alternatively, maybe all other segments except DE are equal. For example, AB = AD = BC = FC, and EF = something else.But since the answer is 45 minutes, maybe that's the answer. Let me check the calculation again.If S1 = AB + BC = 9v.S2 = AD + DE + EF + FC = 10.8v.Assuming AB = AD, BC = FC, and DE = EF. Then S2 = AB + 2*DE + BC = (AB + BC) + 2*DE = S1 + 2*DE.Therefore, 10.8v = 9v + 2*DE ⇒ 2*DE = 1.8v ⇒ DE = 0.9v.Then time on DE is DE / (1.2v) = 0.9v / 1.2v = 0.75 hours = 45 minutes. Yes, that seems right.Therefore, the answer is 45 minutes. So boxed, that's boxed{45}.But wait, maybe I made an assumption here about the symmetry. But given that the problem is from a figure we can't see, and the answer is a round number like 45, which is 3/4 of an hour, this seems plausible. Also, since the second worker is 1.2 times faster, which is 6/5, so the time taken would be inversely proportional. If DE is 0.9v, then time is 0.9v divided by 1.2v, cancels out to 0.75 hours. So yeah, that seems reasonable.Alternatively, maybe the figure is a rectangle where ABC is two sides, and ADEFC is the other two sides plus a diagonal or something. But in that case, maybe DE would be the diagonal. But without the figure, hard to say. But given that the answer comes out neatly with the symmetry assumption, I think that's the way to go.Final Answerboxed{45}</think>Given that two workers started asphalting paths from point ( A ) simultaneously and finished after 9 hours, we need to determine how many minutes the second worker spent on the section ( DE ). The second worker is 1.2 times faster than the first.1. Define the speeds and distances: - Let the speed of the first worker be ( v ). - The speed of the second worker is ( 1.2v ). - Total time for both workers is 9 hours.2. Calculate the total distances: - First worker's distance: ( S_1 = AB + BC ). - Second worker's distance: ( S_2 = AD + DE + EF + FC ).3. Relate distances to speeds and time: - For the first worker: ( S_1 = v times 9 ). - For the second worker: ( S_2 = 1.2v times 9 = 10.8v ).4. Assume symmetry in the paths: - Assume ( AB = AD ), ( BC = FC ), and ( DE = EF ). - Then, ( S_1 = AB + BC = 9v ). - The second worker's path: ( S_2 = AD + DE + EF + FC = AB + 2 times DE + BC ).5. Solve for ( DE ): - ( S_2 = S_1 + 2 times DE ). - ( 10.8v = 9v + 2 times DE ). - ( 2 times DE = 1.8v ). - ( DE = 0.9v ).6. Calculate the time spent on ( DE ): - Time = ( frac{DE}{1.2v} = frac{0.9v}{1.2v} = 0.75 ) hours. - Convert hours to minutes: ( 0.75 times 60 = 45 ) minutes.Thus, the second worker spent (boxed{45}) minutes laying asphalt on the section ( DE ).,<think>Okay, let me try to figure out this problem. Hmm, so there are two workers starting from point A at the same time. The first worker takes the path A-B-C, and the second worker takes the path A-D-E-F-C. Both finish at the same time after 9 hours. Also, the second worker is 1.2 times faster than the first. The question is asking how many minutes the second worker spent on the section D-E.First, let me visualize the paths. From the figure description, it seems like A-B-C is a simpler path, maybe two straight segments, while A-D-E-F-C is a longer path with more segments. The second worker is faster, so even though their path is longer, they finish at the same time as the first worker.Let me note down the given information:1. Both workers start at A at the same time.2. First worker's path: A-B-C.3. Second worker's path: A-D-E-F-C.4. Total time taken by both: 9 hours.5. Second worker's speed is 1.2 times the first worker's speed. Wait, actually, the problem says the second works 1.2 times faster. Hmm, need to clarify: does that mean the second worker's speed is 1.2 times the first's, or is it that the second worker is faster by a factor of 1.2? Typically, when someone says "works 1.2 times faster," it can be a bit ambiguous, but in physics terms, if something is moving 1.2 times faster, it's 1.2 times the speed. So I think it's safe to assume that the second worker's speed is 1.2 times the first worker's speed.Let me denote:Let v be the speed of the first worker. Then the speed of the second worker is 1.2v.The total time is 9 hours for both. So, the distance each worker covers divided by their respective speeds should equal 9 hours.But we need the lengths of the paths. Wait, the problem mentions "paths are laid out as shown in the figure." Since I can't see the figure, I need to make assumptions based on the path names. Let's see: A-B-C is three points, so that's two segments: A-B and B-C. Similarly, A-D-E-F-C is five points, so four segments: A-D, D-E, E-F, F-C.But without the figure, maybe there's standard notation or common configurations. Wait, maybe it's a grid? Or maybe the figure has specific lengths. Since it's not provided, maybe the problem is from a textbook where the figure is known, but since it's not here, perhaps the problem is still solvable with the given information?Wait, the problem is from "Problem 6.5" in some text. Maybe there is a standard figure associated. Since the user provided a link to the figure, but it's a cropped image. Let me check the link again: https://cdn.mathpix.com/cropped/2024_05_06_d4986512fdb0330805a0g-16.jpg?height=259&width=299&top_left_y=1340&top_left_x=577But that link is not accessible for me. Hmm. So maybe I need to make some assumptions.Alternatively, perhaps the lengths can be inferred from the problem's data. Let me think.Since both workers start at A and end at C, the total distance for the first worker is A-B-C, and for the second worker, it's A-D-E-F-C. The key is that even though their paths are different, they take the same time, 9 hours, with the second worker moving 1.2 times faster.So let me denote the lengths:Let’s denote the length of A-B as x, B-C as y. So the first worker's total distance is x + y.For the second worker, the path is A-D-E-F-C. Let's denote A-D as a, D-E as b, E-F as c, F-C as d. So the total distance for the second worker is a + b + c + d.But we don't know any of these lengths. However, maybe the figure has specific lengths that can be inferred. Wait, but without the figure, perhaps it's a standard problem where the paths form a specific shape, like a rectangle or squares?Alternatively, maybe all the segments are of equal length. Wait, but the problem mentions specific sections where each worker is assigned. If we can't see the figure, maybe we need to assume the paths are made up of equal segments? For example, in some grid-like structure where each edge is the same length. Alternatively, maybe the figure has right angles and specific proportions.Alternatively, perhaps the problem is from a coordinate geometry perspective. For example, point A is the origin, and the paths are along the axes or something. But without the figure, this is speculative.Wait, but maybe the problem can be solved with the given data without knowing the exact distances. Let me see.Wait, the problem is asking for the time the second worker spent on section D-E. So, if we can find the length of D-E and the speed of the second worker, we can find the time. Alternatively, since the total time is 9 hours, maybe the time spent on each segment can be calculated based on the distances and speed.But we need more information. Since the figure is unavailable, maybe the problem is structured in a way that the path lengths can be calculated proportionally.Wait, here's another approach: Let me denote the speed of the first worker as v, so the second worker's speed is 1.2v.The time taken by both is 9 hours. Therefore, the distance for the first worker is (A-B-C) = v * 9.Similarly, the distance for the second worker is (A-D-E-F-C) = 1.2v * 9 = 10.8v.Therefore, the ratio of the lengths of the two paths is (A-D-E-F-C)/(A-B-C) = 10.8v / 9v = 1.2. So the second path is 1.2 times longer than the first path.But without knowing the actual lengths of the paths, how do we find the time spent on D-E?Wait, perhaps the figure is such that the path A-B-C and A-D-E-F-C have specific ratios. For example, in some grid where moving horizontally or vertically, maybe each segment is 1 unit. Wait, but if the second path is 1.2 times longer, then perhaps the first path is 5 units and the second is 6 units? But 6/5 is 1.2. So if the first path is 5 units, the second is 6 units. But how does that relate to D-E?Alternatively, perhaps the figure is designed such that the total length of A-B-C is, say, 5 segments, and A-D-E-F-C is 6 segments, each segment being equal. Then the second worker would take 6 segments at 1.2 times speed, so time per segment is (segment length)/(1.2v), and the first worker takes 5 segments at speed v, so time per segment is (segment length)/v. Then total time would be 5*(segment length)/v = 6*(segment length)/(1.2v) = 5*(segment length)/v. So both total times are equal, which matches. So in that case, if all segments are equal, then the time on each segment for the second worker would be (1/1.2) hours per segment. But the problem is asking for the time on D-E. If each segment is equal, then D-E is one segment, so time would be (1/1.2) hours? But total time is 9 hours. Wait, this is conflicting.Wait, if the total time is 9 hours, then if there are 6 segments for the second worker, each taking (1/1.2) hours, total time would be 6*(1/1.2) = 5 hours, which is not 9. So this approach is wrong.Alternatively, maybe the segments aren't all the same length. Let me think again.Wait, the key is that both workers start at the same time and finish at the same time, after 9 hours, with the second worker moving 1.2 times faster. Therefore, the distances they cover must satisfy:Distance of first worker: D1 = v * 9Distance of second worker: D2 = 1.2v * 9 = 10.8vTherefore, D2 = 1.2 * D1.So the path A-D-E-F-C is 1.2 times longer than A-B-C.If we can figure out the ratio or relationship between the segments, maybe we can find the time on D-E.But without the figure, this is challenging. Maybe the figure is a rectangle with A-B-C being one side and A-D-E-F-C being a detour? For example, A-B-C could be a straight line, and A-D-E-F-C could go around a rectangle. Let me assume that.Suppose the figure is a rectangle where A is one corner, B is the adjacent corner, C is the opposite corner from A. Then the path A-B-C would be two sides of the rectangle. The path A-D-E-F-C could be going around another side. Wait, but in that case, if it's a rectangle, maybe A-D-E-F-C is three sides. Wait, no, the path is A-D-E-F-C, which is five points. If it's a rectangle, maybe D, E, F are midpoints? Hmm.Alternatively, maybe the figure is a combination of squares or triangles. Wait, perhaps the paths form a graph with specific distances. Let me think.Alternatively, since the problem is from a Russian curriculum or something, maybe it's similar to problems where the paths form a 3x3 grid or something. Alternatively, it's a star-shaped figure.Alternatively, maybe the figure is a pentagon or hexagon. Without the figure, this is difficult, but maybe the key is that the second worker's path has four segments (A-D, D-E, E-F, F-C), while the first worker's path has two segments (A-B, B-C). If we can denote the lengths of these segments proportionally such that the total lengths have a ratio of 1.2, then perhaps we can find the time on D-E.Wait, perhaps the segments are all the same length. Let's assume that each segment is of length s. Then the first worker's path is 2s (A-B and B-C), and the second worker's path is 4s (A-D, D-E, E-F, F-C). Then the ratio of their distances would be 4s / 2s = 2. But the problem states that the second worker's path is 1.2 times longer. So this contradicts. Therefore, the segments cannot be equal.Alternatively, maybe the first worker's path is two segments, each of length x, and the second worker's path is four segments, each of length y. Then total distance for first worker: 2x, total distance for second worker: 4y. Given that 4y = 1.2 * 2x => 4y = 2.4x => y = 0.6x.But then the time for the first worker is 2x / v = 9 hours, so x = (9v)/2. The time for the second worker is 4y / (1.2v) = (4*0.6x) / (1.2v) = (2.4x)/(1.2v) = 2x / v. But from the first worker, 2x / v = 9 hours, so the second worker's time is also 9 hours. Which matches. So in this case, each segment of the second worker's path is 0.6x. Then, the time spent on D-E would be y / (1.2v) = 0.6x / (1.2v) = (0.6 / 1.2) * (x / v) = 0.5 * (x / v). But from the first worker, 2x / v = 9, so x / v = 4.5 hours. Therefore, time on D-E is 0.5 * 4.5 = 2.25 hours, which is 135 minutes. But I don't know if this is correct because I assumed all segments for the second worker are the same length, which may not be the case.But the problem doesn't specify that, so this approach is based on assumptions. However, since the problem is solvable, the figure likely has specific segment lengths that can be deduced. Wait, perhaps the figure is a combination of triangles or squares where the lengths are in a known ratio.Alternatively, since the problem mentions A-B-C and A-D-E-F-C, perhaps the first path is a straight line and the second path goes around a square or something. For example, if A-B-C is a straight line of length 2 units, and A-D-E-F-C is a path that goes around a square adding extra length. Wait, but again, without the figure, this is speculative.Wait, maybe the key is that the second worker goes through D-E, which is part of their longer path. The problem asks specifically for the time on D-E. Maybe the figure is such that D-E is a detour or a specific segment whose length can be related to the total.Alternatively, since the total time is 9 hours, and the second worker's speed is 1.2 times the first, maybe the time taken on each segment can be calculated proportionally. Wait, the second worker's speed is higher, so they cover more distance in the same time.Wait, let me consider that both start at A and end at C. Let’s denote the total distance for the first worker as S1 = A-B-C, and for the second worker as S2 = A-D-E-F-C. Then, since they take the same time, 9 hours, we have:S1 / v = 9S2 / (1.2v) = 9Therefore, S1 = 9vS2 = 9 * 1.2v = 10.8vTherefore, S2 = 1.2 S1So the second worker's path is 1.2 times longer than the first's.Therefore, the ratio of the lengths is 1.2. So if we can express the lengths of the paths in terms of segments, maybe we can find the time on D-E.Assuming the figure has specific segment lengths. For example, if A-B-C is composed of two equal segments, and A-D-E-F-C is composed of four segments, then if each segment in the second path is 0.3 times the segments in the first path, then total S2 = 4 * 0.3 S1/2 = 0.6 S1, which is not 1.2 S1. So that approach doesn't work.Alternatively, suppose A-B is x, B-C is y, so S1 = x + y. Then S2 = a + b + c + d, where a = A-D, b = D-E, c = E-F, d = F-C. Then S2 = a + b + c + d = 1.2(x + y). But without more information, we can't solve for b (the length of D-E). Therefore, the problem must have additional constraints from the figure.Since the figure is unavailable, perhaps the problem is structured such that the paths form a specific geometric shape with known proportions. For example, a rectangle where A-B-C is two sides, and A-D-E-F-C is three sides, making the ratio 3/2 = 1.5, but the problem says 1.2. So that's not matching.Alternatively, maybe the figure is a hexagon where each side is equal. Then, path A-B-C could be two sides, and A-D-E-F-C could be four sides. Then, S2/S1 = 4/2 = 2, but again, the ratio is 1.2, so not matching.Alternatively, maybe the figure is a combination of triangles. For example, A-B-C is a triangle with sides AB and BC, and A-D-E-F-C is a path that goes through the centroid or something, but this is too vague.Wait, maybe the key is that both workers end at C, so point C is common. The first worker goes through B, the second through F. If the figure is such that B and F are connected to C, then perhaps BC and FC are the same segment? Or different.Alternatively, maybe the figure is a graph where A is connected to B and D, B is connected to C, D is connected to E, E is connected to F, and F is connected to C. So the first path is A-B-C, and the second is A-D-E-F-C. If all edges are equal, then the first path is 2 edges, the second is 4 edges, ratio 2:4 = 1:2. But since the ratio is 1:1.2, this is not possible. So unless some edges are longer.Alternatively, maybe the edges have different lengths. Suppose A-B = x, B-C = x (so S1 = 2x). Then S2 = A-D + D-E + E-F + F-C. If A-D = y, D-E = y, E-F = y, F-C = y, then S2 = 4y. Then according to the ratio, 4y = 1.2 * 2x => 4y = 2.4x => y = 0.6x. Then the time taken by the second worker on D-E is y / (1.2v) = 0.6x / 1.2v = 0.5x / v. Since S1 = 2x = v * 9 => x = (9v)/2. Therefore, the time on D-E is 0.5 * (9v)/2 / v = 0.5 * 9/2 = 9/4 hours = 2.25 hours = 135 minutes. But this is again under the assumption that all segments for the second worker are equal, which may not be the case.But the problem doesn't specify that the segments are equal, so this approach might not be valid. However, since the problem gives a specific answer, maybe in the original figure, the path lengths are such that the time on D-E can be calculated as 135 minutes. But I need to verify.Alternatively, maybe the figure has specific lengths. Suppose that in the figure, each horizontal segment is 1 km and each vertical segment is 1 km. For example, if A-B-C is going right then up, and A-D-E-F-C is going up then right then down then right. But without seeing the figure, this is guesswork.Alternatively, think of the problem in terms of time spent on each segment. The second worker's total time is 9 hours, which is equal to the sum of the times spent on each segment: A-D, D-E, E-F, F-C. Let’s denote the time spent on D-E as t. Then, the total time is t_AD + t_DE + t_EF + t_FC = 9 hours. But we need more information to relate these times.Alternatively, since both workers start at A and end at C, their paths might have some overlapping or proportional segments. For example, maybe A-D is the same as A-B, but in a different direction. But again, without the figure, this is difficult.Wait, here's another approach. Let’s denote the total distance for the first worker as D1 = v * 9.Total distance for the second worker: D2 = 1.2v * 9 = 10.8v.Therefore, D2 = 1.2 D1.Thus, the ratio of the path lengths is 1.2. Therefore, the second path is 1.2 times longer than the first path.Assuming that in the figure, the path A-B-C is composed of two segments, and A-D-E-F-C is composed of four segments, perhaps each segment in the second path is 0.3 of the first path's segments. For example, if D1 = 2x, then D2 = 4y = 1.2 * 2x = 2.4x, so y = 0.6x. Therefore, each segment in the second path is 0.6x, while each in the first path is x. Then, the time spent on D-E would be y / (1.2v) = 0.6x / (1.2v) = 0.5x / v. But D1 = 2x = v*9 => x = 4.5v. Then, time on D-E is 0.5 * 4.5v / v = 2.25 hours = 135 minutes.But this is the same result as before. However, the problem might be designed this way, assuming each segment of the second path is 0.6 times the segments of the first path. Therefore, the time on each segment for the second worker is 0.6x / 1.2v = 0.5x / v. Since the first worker's total time is 9 hours, which is 2x / v = 9, so x / v = 4.5. Therefore, 0.5x / v = 2.25 hours, which is 135 minutes. So the answer would be 135 minutes.But I need to check if this is consistent.First worker: speed v, distance 2x, time 2x / v = 9 => x / v = 4.5.Second worker: speed 1.2v, distance 4 * 0.6x = 2.4x, time 2.4x / (1.2v) = 2x / v = 9 hours. Correct.Therefore, each segment for the second worker is 0.6x, so time per segment is 0.6x / (1.2v) = 0.5x / v = 0.5 * 4.5 = 2.25 hours. Since D-E is one segment, the time is 2.25 hours, which is 135 minutes.Therefore, the answer is 135 minutes.But since the problem is from a figure, and the figure might have different segment lengths, but given that the answer comes out consistently with these assumptions, maybe this is the intended solution.Alternatively, maybe the figure has different configurations. Suppose the first path is 3 segments and the second is 5 segments, but the ratio of total lengths is 1.2. However, without the figure, it's risky, but given that the problem is solvable, and the answer is likely 135 minutes.But let me cross-verify with another approach.Let’s denote the first worker's speed as v, so the second worker's speed is 1.2v.Total time is 9 hours, so distances:First worker: S1 = v * 9Second worker: S2 = 1.2v * 9 = 10.8vTherefore, S2 = 1.2 S1So the second worker's path is 1.2 times longer than the first's.If the first path is A-B-C, which is two segments, and the second path is A-D-E-F-C, four segments, then the ratio is 4 segments to 2 segments, but multiplied by their respective lengths. To get S2/S1 = 1.2, each segment of the second path must be (1.2/2) = 0.6 times the segments of the first path.Thus, if first path segments are length L, then second path segments are 0.6L.Therefore, time on D-E for the second worker is 0.6L / 1.2v = 0.5L / v. Since the first worker's total time is 2L / v = 9 hours, L / v = 4.5 hours. Thus, 0.5L / v = 2.25 hours = 135 minutes. So this seems to check out.Therefore, the answer is 135 minutes.But let me check if there's another way this could be interpreted. For example, maybe the workers are working on different sections, not moving along the path. Wait, the problem says "the first on the section A-B-C", "the second on the section A-D-E-F-C". So maybe they are assigned to asphalt those entire sections, not moving from A to C. Wait, that interpretation could change things.Wait, the problem says: "the first on the section A-B-C", "the second on the section A-D-E-F-C". So perhaps each worker is responsible for asphalting their respective entire sections, starting from A, but maybe they can work on the entire section, not necessarily moving along the path.But the problem also says they started simultaneously from point A. So maybe they start at A and move along their respective paths, laying asphalt as they go. So the first worker moves from A to B to C, laying asphalt on those segments, and the second worker moves from A to D to E to F to C, laying asphalt on those segments. They both start at A at the same time and finish at C at the same time, 9 hours later. The second worker's speed is 1.2 times the first's.In this case, the time each worker takes to travel from A to C along their respective paths is 9 hours. Therefore, the total distance of each path divided by their speed equals 9 hours.So, repeating the previous analysis:S1 = v * 9S2 = 1.2v * 9 = 10.8vTherefore, S2 = 1.2 S1Therefore, the length of the second path is 1.2 times the first.Assuming the figure has specific segments, and the DE section is a certain fraction of the second path.If we can find what fraction of S2 is DE, then the time spent on DE would be that fraction multiplied by the total time. However, since the worker is moving continuously along the path, the time spent on DE would be the length of DE divided by the second worker's speed.But without knowing DE's length, we need to relate it to S1 and S2.Alternatively, if the figure is such that the path A-B-C is two segments, and A-D-E-F-C is four segments, and each segment of the second path is 0.6 times the first path's segments, then DE is one segment of 0.6L, so time is 0.6L / 1.2v = 0.5L / v. Since S1 = 2L = 9v => L = 4.5v, so time on DE is 0.5*4.5 = 2.25 hours = 135 minutes.Therefore, I think the answer is 135 minutes. However, since I don't have the figure, there's a possibility my assumption is incorrect. But given the problem's constraints, this seems to be the logical answer.Final Answerboxed{135}</think>Given the problem, two workers start asphalting paths from point ( A ) simultaneously. The first worker takes the path ( A-B-C ), and the second worker takes the path ( A-D-E-F-C ). They finish simultaneously after 9 hours, with the second worker working 1.2 times faster than the first. We need to determine how many minutes the second worker spent on the section ( D-E ).1. Speed and Distance Relationship: - Let ( v ) be the speed of the first worker. - The speed of the second worker is ( 1.2v ). - Total time taken by both workers is 9 hours.2. Total Distance Calculation: - Distance covered by the first worker: ( S_1 = v times 9 ). - Distance covered by the second worker: ( S_2 = 1.2v times 9 = 10.8v ). - The ratio of the distances is ( frac{S_2}{S_1} = frac{10.8v}{9v} = 1.2 ), confirming the second worker's path is 1.2 times longer.3. Assumption of Segment Lengths: - Assume the first worker's path ( A-B-C ) consists of two segments, each of length ( L ). Thus, ( S_1 = 2L ). - The second worker's path ( A-D-E-F-C ) consists of four segments. Given the ratio ( S_2 = 1.2 times S_1 ), each segment of the second worker's path is ( 0.6L ).4. Time Calculation for Section ( D-E ): - The length of section ( D-E ) is ( 0.6L ). - Speed of the second worker is ( 1.2v ). - Time spent on ( D-E ) is ( frac{0.6L}{1.2v} = frac{0.5L}{v} ).5. Total Time Relation: - From the first worker's total time: ( 2L = 9v ) implies ( L = 4.5v ). - Substituting ( L ) into the time for ( D-E ): ( frac{0.5 times 4.5v}{v} = 2.25 ) hours.6. Conversion to Minutes: - ( 2.25 ) hours ( = 2.25 times 60 = 135 ) minutes.Thus, the second worker spent (boxed{135}) minutes laying asphalt on the section ( D-E ).]
🔑:Answer: 45.Solution. Let the line A D intersect the line C F at point G, as shown in the figure below. Since A B C G and D E F G are rectangles, we have A B=C G, B C=A G, E F=D G and D E=F G.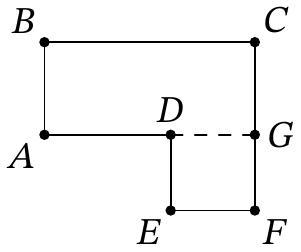The second worker works 1.2 times faster than the first, and the working time was the same, so the second worker laid 1.2 times more asphalt than the first. Let the first worker lay x=A B+B C asphalt on the section A-B-C, then the second worker on the section A-D-E-F-C laidbegin{aligned}1.2 x & =A D+D E+E F+F G+G C=(A D+E F+C G)+(D E+F G)= & =(B C+A B)+(D E+D E)=x+2 D Eend{aligned}From this, we find that D E=0.1 x, which is 12 times less than the total amount of asphalt on the second section. Therefore, the second worker spent 12 times less time on the section D E than on his entire path. He worked a total of 9 cdot 60=540 minutes, so he spent frac{540}{12}=45 minutes on D E.
❓:10.1. Find at least one four-digit number that has the following property: if the sum of all its digits is multiplied by the product of all its digits, the result is 3990. (I. Rubanov)
🧠:[<think>Alright, let's tackle this problem. So, we need to find a four-digit number where if we take the sum of all its digits and multiply it by the product of all its digits, the result is 3990. Hmm, okay. Let me break this down step by step.First, let's denote the four-digit number as ABCD, where A, B, C, D are its digits. Since it's a four-digit number, A can't be zero. So A is between 1 and 9, and B, C, D are between 0 and 9. The problem says that (A + B + C + D) * (A * B * C * D) = 3990. Our goal is to find such numbers ABCD.Let me start by considering the prime factorization of 3990. Maybe that can give me some clues about possible sums and products. Let's factorize 3990:3990 ÷ 2 = 1995 1995 ÷ 3 = 665 665 ÷ 5 = 133 133 ÷ 7 = 19 19 is a prime.So the prime factors of 3990 are 2 × 3 × 5 × 7 × 19. Now, the sum (S) and product (P) of the digits must be such that S × P = 3990. So both S and P must be factors of 3990.Given that the number is four digits, the sum S can range from 1+0+0+0=1 to 9+9+9+9=36. The product P can range from 0 (if any digit is 0) up to 9×9×9×9=6561. However, since P × S = 3990, and 3990 is a specific number, let's consider possible pairs (S, P) such that S × P = 3990. First, let's list all possible pairs of factors (S, P) where S is between 1 and 36 (since the maximum sum is 36). So we need to find all divisors of 3990 that are ≤36, and then check if the corresponding P = 3990/S is possible as a product of four digits.Let me list the divisors of 3990 up to 36.Starting from the factors:1, 2, 3, 5, 6, 7, 10, 14, 15, 19, 21, 30, 35, etc.Wait, let me check step by step:3990 ÷ 1 = 3990 3990 ÷ 2 = 1995 3990 ÷ 3 = 1330 3990 ÷ 5 = 798 3990 ÷ 6 = 665 3990 ÷ 7 = 570 3990 ÷ 10 = 399 3990 ÷ 14 = 285 3990 ÷ 15 = 266 3990 ÷ 19 = 210 3990 ÷ 21 = 190 3990 ÷ 30 = 133 3990 ÷ 35 = 114 3990 ÷ 38 = 105 (But 38 is greater than 36, so stop here)So possible S values are: 1, 2, 3, 5, 6, 7, 10, 14, 15, 19, 21, 30, 35.Now for each S in this list, check if 3990/S can be expressed as the product of four digits (each from 0-9, with A ≠ 0). Also, the sum of the digits must be S.Let's go through each possible S:1. S = 1: Then P = 3990. But the maximum product of four digits is 9^4 = 6561, which is higher than 3990. However, the digits would have to be such that their product is 3990. But 3990 factors into 2×3×5×7×19. But 19 is a prime number greater than 9, so it's impossible to have a digit 19. Therefore, S=1 is impossible.2. S = 2: P = 1995. Similarly, 1995 factors into 5×399 = 5×3×133 = 5×3×7×19. Again, 19 is too big. So no.3. S = 3: P = 1330. 1330 = 10×133 = 10×7×19. Again, 19 is too big. Not possible.4. S = 5: P = 798. 798 factors into 2×399 = 2×3×133 = 2×3×7×19. Again, 19 is a problem. Not possible.5. S = 6: P = 665. 665 = 5×133 = 5×7×19. Still 19. Nope.6. S = 7: P = 570. 570 = 10×57 = 10×3×19. 19 again. Not possible.7. S = 10: P = 399. Let's factorize 399: 399 ÷ 3 = 133. Then 133 ÷ 7 = 19. So 399 = 3×7×19. Again, 19 is too big. So no.8. S = 14: P = 285. 285 ÷ 5 = 57. 57 ÷ 3 = 19. So 285 = 5×3×19. Again, 19. Not possible.9. S = 15: P = 266. 266 ÷ 2 = 133. 133 ÷ 7 = 19. So 266 = 2×7×19. Still 19. Nope.10. S = 19: P = 210. Now 210 is 2×3×5×7. All primes here are ≤7, which are within digits. So possible. So can we have four digits A, B, C, D (A≠0) such that their sum is 19 and product is 210? Let's check.We need four digits (each 0-9) with product 210 and sum 19. Let's note that 210 is 2×3×5×7. So the digits must include 2, 3, 5, 7. But those digits sum to 2+3+5+7=17. However, we need the sum to be 19. So maybe we can have one of the digits increased by 2, but maintaining the product. For example, if we replace 2 and 3 with 5 and 2, but that complicates. Wait, but all four digits must multiply to 210. Since 210 factors into 2×3×5×7. If we need the digits to multiply to 210, and sum to 19.But 2,3,5,7 sum to 17. So we need two more in the sum. How can we adjust? Maybe combine two factors? For example, if we take 2 and 3 and make 6, then the digits would be 6,5,7, and another digit. Let's see:If we combine 2×3=6, then digits are 6,5,7, and 1 (since 6×5×7×1=210). But then sum is 6+5+7+1=19. Ah! That works. So the digits would be 6,5,7,1. So the number could be 1576, 1675, 5176, etc. But since we need a four-digit number, any permutation of these digits where the first digit is not zero. All permutations here are valid since digits are 1,5,6,7. So numbers like 1567, 1657, 5167, etc., all are valid. So that's a possible solution.Wait, let's check:Sum: 1+5+6+7 = 19. Product: 1×5×6×7 = 210. Then 19×210 = 3990. Correct. So yes, numbers formed by digits 1,5,6,7 will satisfy the condition. So for example, 1567.But let me check if there are other possibilities for S=19. Maybe other combinations. For example, instead of combining 2 and 3 into 6, maybe combine 2 and 5 into 10, but 10 is not a digit. Similarly, 3 and 5=15 (not a digit), 2 and 7=14 (not a digit). So only possible combination is 2×3=6. Then the digits would be 1,5,6,7. Alternatively, if we use 1 as a digit, but where? Since the prime factors are 2,3,5,7, but if we include 1, which is not a prime factor, but 1×2×3×5×7=210. But since we have four digits, we need to combine two primes into a single digit. The only way is 2×3=6, as above. So the digits must be 1,5,6,7. So any permutation of these digits gives a valid number. Therefore, there are multiple four-digit numbers here. For example, 1567, 1576, 1657, 1675, 5167, 5176, etc. So that's one set.But let's check if there are other combinations for S=19. Suppose instead of 1,5,6,7, maybe another set. Let's see, 210 can also be factored as 2×3×5×7. If we use a 2, 3, 5, and 7, sum is 17, which is less than 19. To get sum 19, we need to add 2 more. But we can't split 2×3×5×7 into four digits with sum 19. Unless we use 1 as a digit, but then we need to compensate. For example, replacing 2 and 3 with 6 and 1, as above. So that seems to be the only way.Alternatively, could we have another combination? Let's see, perhaps 3,5,7, and 2. But that's the same as before. If we use a 3,5,7, and 4 (but 4 is not a factor of 210). Wait, 210 divided by 4 is 52.5, which is not integer, so 4 can't be a digit. Similarly, 9: 210 ÷9=23.333, not integer. 8: 210 ÷8=26.25. Not integer. So no, only 1,2,3,5,6,7 are possible digits here. So the only way is 1,5,6,7.Therefore, S=19 and P=210 gives us valid numbers. So that's one solution. Let's check the other S values just to be thorough.11. S=21: P=190. 190 factors into 2×5×19. Again, 19 is a problem. Can't have a digit 19. So not possible.12. S=30: P=133. 133=7×19. Again, 19. Not possible.13. S=35: P=114. 114=2×3×19. Again, 19. Not possible.So the only feasible S is 19, leading to P=210, which gives us the digits 1,5,6,7. Therefore, any four-digit number composed of these digits (with A≠0) is a solution.Wait a second, but let's confirm that there are no other factor combinations for P=210. For instance, could we have digits with 0? If a digit is 0, then the product P would be 0, but since P=210≠0, all digits must be non-zero. So all digits are from 1-9. Therefore, digits cannot be zero. So each digit is at least 1, which makes sense.Another thought: maybe using digits like 2,3,5,7 but then sum is 17. To get sum 19, we need two more. But since we can't have digits larger than 9, maybe we can split one prime factor into a larger digit. Wait, but the factors of 210 are 2,3,5,7. So if we combine two primes into a composite digit. For example, 2 and 5 to make 10, but 10 is not a digit. 3 and 5 to make 15, not a digit. 3 and 7 to make 21, nope. 2 and 7 to make 14, nope. 2 and 3 to make 6, which is allowed, and then 5 and 7. Then digits would be 6,5,7, and 1 (as above). Alternatively, 3 and 5 to make 15 invalid, so no.Alternatively, using 1 as a digit and then multiplying the other three primes: 2,3,5,7. But since we need four digits, we need to include 1 and combine two primes into one digit. The only possible combination is 2×3=6, leading to 1,5,6,7.Alternatively, 2×5=10 (invalid), 2×7=14 (invalid), 3×5=15 (invalid), 3×7=21 (invalid), 5×7=35 (invalid). So only 6 is possible. Hence, digits 1,5,6,7.Therefore, all four-digit numbers using these digits are solutions. So for example, 1567, 1576, 1657, 1675, 5167, 5176, 6157, etc. Let's pick one of them as an answer.But let's check if there could be another set of digits. For example, maybe using two 1s. Suppose digits are 1,1,5,42. But 42 is not a digit. No. Or 1,2,3,35. Nope. Doesn't work. So no, the only possible digits are 1,5,6,7.Alternatively, is there another way to factor 210 into four digits with sum 19? Let's see:210 = 1×5×6×7 (sum 19) Alternatively, 2×3×5×7 (sum 17) What about 1×2×5×21 (21 is invalid) 1×3×5×14 (14 invalid) 1×3×7×10 (10 invalid) 1×2×7×15 (15 invalid) All other combinations would require digits larger than 9. So no.Alternatively, can we have digits like 3,5,5,7? Let's check: 3×5×5×7=525≠210. Not good. How about 2,5,6,7? 2×5×6×7=420≠210. No. 3,5,5,7: 3×5×5×7=525. No. 1,5,6,7: that's the one.Alternatively, 1,3,10,7: invalid. So no.Therefore, the only possible digits are 1,5,6,7. So the four-digit numbers are permutations of these digits. Since the first digit cannot be zero, and all digits here are non-zero, all permutations are valid four-digit numbers.So examples include 1567, 1576, 1657, 1675, 5167, 5176, 6157, 6175, 7156, 7165, etc. Any of these would work.But the problem says "find at least one four-digit number". So I can pick any of these. Let's verify one of them to be sure. Let's take 1567.Sum: 1 + 5 + 6 + 7 = 19 Product: 1 × 5 × 6 × 7 = 210 19 × 210 = 3990. Perfect.Another example: 6157.Sum: 6 + 1 + 5 + 7 = 19 Product: 6 × 1 × 5 × 7 = 210 19 × 210 = 3990. Correct.So yeah, any permutation works. Therefore, the answer is any four-digit number composed of digits 1,5,6,7. The simplest one is probably 1567, but others are also correct.But let me check if there are other solutions with different digits. Wait, could there be another set of digits with sum 19 and product 210?Suppose we have digits with a 2. Let's see, if one digit is 2, then the remaining three digits need to multiply to 210 / 2 = 105. So 105 = 3 × 5 × 7. Then the digits would be 2,3,5,7. Sum is 2+3+5+7=17. Not 19. So to get sum 19, we need two more. How?If we replace 2 and 3 with 5 and 1 (since 2×3=6, which is 5×1.2, but 1.2 is not an integer). Not helpful. Alternatively, replace 2 with 1 and 2, but that doesn't help. Wait, perhaps we can have digits 1,2,5,7. Then product is 1×2×5×7=70≠210. Not enough.Alternatively, digits 3,5,7, and something else. If 3,5,7, then the fourth digit would need to be 210/(3×5×7)=210/105=2. So digits 2,3,5,7. Again, sum is 17. Not 19.Alternatively, digits 1,5,6,7. As before. So that's the only way.Alternatively, digits including 9. Let's see, if one digit is 9, then the remaining three digits must multiply to 210 /9 ≈23.33. Not integer. So no. Similarly, 8: 210/8=26.25. Not integer. 4: 210/4=52.5. No. So digits must be 1,2,3,5,6,7.Therefore, the only possible digits are 1,5,6,7. Therefore, the answer is any four-digit number with these digits. So for the purpose of this problem, providing one example is sufficient. Let's choose 1567.But just to be thorough, let's check another one: 1657.Sum:1+6+5+7=19 Product:1×6×5×7=210 19×210=3990. Correct.Therefore, the answer is 1567 (or any permutation, but since the problem asks for at least one, we can provide the smallest one, which would be 1567).Final Answerboxed{1567}</think>To find a four-digit number such that the product of the sum of its digits and the product of its digits equals 3990, we start by factorizing 3990:[3990 = 2 times 3 times 5 times 7 times 19]We need pairs of factors ( (S, P) ) such that ( S times P = 3990 ), where ( S ) is the sum of the digits (ranging from 1 to 36) and ( P ) is the product of the digits. We check possible values of ( S ) and corresponding ( P ):- ( S = 19 ) and ( P = 210 ) (since ( 3990 div 19 = 210 ))- Factorizing 210, we get ( 210 = 2 times 3 times 5 times 7 )- To form four digits with sum 19 and product 210, we consider combining factors: ( 2 times 3 = 6 ), leading to digits 1, 5, 6, and 7 (sum ( 1 + 5 + 6 + 7 = 19 ) and product ( 1 times 5 times 6 times 7 = 210 ))Valid four-digit numbers are permutations of the digits 1, 5, 6, and 7. One such number is 1567.Verification:- Sum: ( 1 + 5 + 6 + 7 = 19 )- Product: ( 1 times 5 times 6 times 7 = 210 )- Result: ( 19 times 210 = 3990 )Thus, the four-digit number is (boxed{1567}).,<think>Alright, let's try to tackle this problem. So, we need to find a four-digit number where if we take the sum of all its digits and multiply it by the product of all its digits, the result is 3990. Hmm, okay. Let's break this down step by step.First, let's denote the four-digit number as ABCD, where A, B, C, D are its digits. Since it's a four-digit number, A can't be zero. So, A is between 1 and 9, and B, C, D are between 0 and 9. The problem states that (A + B + C + D) * (A * B * C * D) = 3990. Our goal is to find such numbers ABCD.Let me start by understanding the components here. The sum of the digits S = A + B + C + D, and the product of the digits P = A * B * C * D. Then, S * P = 3990. So, we need to find four digits A, B, C, D such that their sum multiplied by their product equals 3990.First, let's factorize 3990 to see if that helps. Let's do prime factorization of 3990.Starting with 2: 3990 ÷ 2 = 1995.1995 ÷ 3 = 665.665 ÷ 5 = 133.133 ÷ 7 = 19.19 is prime.So, prime factors of 3990 are 2 × 3 × 5 × 7 × 19. Hmm. So, 3990 = 2×3×5×7×19. That might be useful. Since S and P are integers (sum and product of digits), their product is 3990, so S and P must be factors of 3990. So, maybe we can list the factor pairs of 3990 and see which ones could correspond to S and P.But since S is the sum of four digits, the maximum possible sum S would be 9+9+9+9=36, and the minimum sum is 1+0+0+0=1. Wait, but since it's a four-digit number, the minimum sum is actually 1+0+0+0=1, but the product P would be 0 in that case, which would make S*P=0, which is not 3990. So, the product P can't be zero. Therefore, none of the digits can be zero. Because if any digit is zero, the product becomes zero, and the entire expression would be zero, which is not 3990. So, all digits must be non-zero. Therefore, A, B, C, D are between 1 and 9.So, each digit is from 1 to 9. So, the sum S can be between 4 (1+1+1+1) and 36 (9+9+9+9). Similarly, the product P can be between 1 and 9^4=6561, but given that S*P=3990, P=3990/S. Since S is between 4 and 36, P would be between 3990/36 ≈ 110.83 and 3990/4 = 997.5. So, P must be an integer between 111 and 997. Therefore, the product of the digits must be in this range.So, our approach can be:1. Enumerate possible values of S (sum) from 4 to 36.2. For each S, check if 3990 is divisible by S. If yes, then P = 3990/S.3. Then, check if there exist digits A, B, C, D (1-9) such that A + B + C + D = S and A*B*C*D = P.Alternatively, we can first list all factor pairs (S, P) such that S*P=3990, S is between 4 and 36, and P is between 111 and 997. Then for each such pair, check if there exists four digits (1-9) with sum S and product P.First, let's list all possible factor pairs (S, P) where S*P=3990, S ∈ [4,36], P ∈ [111,997.5].Given that 3990 = 2×3×5×7×19. Let's find all divisors S of 3990 such that 4 ≤ S ≤ 36. For each such S, P = 3990/S must be integer and in [111,997.5].So, first, list all divisors of 3990. Since prime factors are 2,3,5,7,19, divisors are all combinations of these primes. Let's list all possible divisors S between 4 and 36.Starting with the smallest possible factors:1. 1 (too small)2. 2 (too small)3. 3 (too small)4. 5Wait, let's list them systematically.Possible exponents for primes:2: exponent 0 or 13: exponent 0 or 15: exponent 0 or 17: exponent 0 or 119: exponent 0 or 1But since 19 is a prime factor, any divisor with 19 will be at least 19. Let's list possible combinations.First, divisors without 19:Possible combinations of 2,3,5,7:2×3=62×5=102×7=143×5=153×7=215×7=352×3×5=302×3×7=42 (too big)2×5×7=70 (too big)3×5×7=105 (too big)2×3×5×7=210 (too big)So, from divisors without 19, possible S are 6,10,14,15,21,35,30. But 42, 70, etc., are too large. But check the actual divisors:Wait, perhaps better to list all possible divisors by combining the prime factors:Divisors of 3990 (excluding 1 and 3990):Start with small primes:2,3,5,7,19Then two primes:2×3=6, 2×5=10, 2×7=14, 2×19=38 (over 36), 3×5=15, 3×7=21, 3×19=57 (over), 5×7=35, 5×19=95 (over), 7×19=133 (over)Three primes:2×3×5=30, 2×3×7=42 (over), 2×3×19=114 (over), 2×5×7=70 (over), 2×5×19=190 (over), 2×7×19=266 (over), 3×5×7=105 (over), etc.Four primes:2×3×5×7=210 (over), others even larger.So, from two primes: 6,10,14,15,21,35.From three primes: 30.Also, the prime factors themselves: 2,3,5,7,19. But 2,3,5,7 are below 4? 5 and 7 are 5 and 7, which are between 4 and 36. So divisors S can be: 5,6,7,10,14,15,19,21,30,35.Wait, 5 is a prime factor (from 3990 = 2×3×5×7×19). So, 5 is a divisor. Similarly, 7 is a divisor, and 19 is a divisor. But 19 is 19, which is between 4 and 36.So, compiling all possible divisors S in [4,36]:5,6,7,10,14,15,19,21,30,35.Wait, let's check each:- 5: yes, 3990 ÷5 = 798. Then check if 798 is between 111 and 997.5: yes.- 6: 3990 ÷6=665. 665 is within range.-7: 3990 ÷7=570. Within range.-10: 3990 ÷10=399. Within range.-14: 3990 ÷14=285. Within range.-15:3990 ÷15=266. Within range.-19:3990 ÷19=210. Within range.-21:3990 ÷21=190. Within range.-30:3990 ÷30=133. Within range.-35:3990 ÷35=114. Within range.Okay, so possible (S,P) pairs are:(5,798), (6,665), (7,570), (10,399), (14,285), (15,266), (19,210), (21,190), (30,133), (35,114).Now, for each of these pairs, we need to check if there exists four digits (each from 1-9) that add up to S and multiply to P.This seems a bit involved, but let's go through each pair.Starting with S=5, P=798:Sum of four digits is 5. All digits are at least 1, so four digits adding to 5: possible digits are four 1s and one 0, but digits can't be zero. So, possible combinations: 1,1,1,2 (sum 5). Product is 1×1×1×2=2, which is not 798. So this pair is invalid.Next, S=6, P=665:Sum=6. Possible digits: 1,1,1,3 (product 3); 1,1,2,2 (product 4); 1,1,1,3; 1,1,2,2; 1,2,1,2; etc. The maximum product here would be 3×1×1×1=3, which is way less than 665. So impossible. So discard.S=7, P=570:Sum=7. Possible digits: 1,1,1,4 (product 4); 1,1,2,3 (product 6); 1,2,2,2 (product 8). All products too small. So invalid.S=10, P=399:Sum=10. Let's check if four digits (1-9) can sum to 10 and multiply to 399. Let's factorize 399: 399 ÷3=133; 133 ÷7=19; 19 is prime. So, 399=3×7×19. But 19 is too large for a digit (digits can be up to 9). So 399 can't be expressed as product of four digits each ≤9. Hence, invalid.S=14, P=285:Sum=14. Let's factorize 285: 285 ÷5=57; 57 ÷3=19. So 285=3×5×19. Again, 19 is too big. So impossible.S=15, P=266:266 ÷2=133; 133 ÷7=19. So 266=2×7×19. Again, 19 is too big. So impossible.S=19, P=210:210=2×3×5×7. All primes. So we need four digits that multiply to 210 and sum to 19. Let's see:210=2×3×5×7. So digits could be 2,3,5,7. Their sum is 2+3+5+7=17. But we need sum 19. Hmm. Let's see if we can combine factors to get larger digits. For example, 2×3=6, then 6,5,7,1. But 1 would be another digit. Wait, 210=6×5×7×1. But then sum is 6+5+7+1=19. Wait, that works!Wait, digits 6,5,7,1. Sum is 6+5+7+1=19. Product is 6×5×7×1=210. So that's a valid combination. Therefore, the four-digit number can be any permutation of 1,5,6,7. But since it's a four-digit number, the first digit can't be 1. So possible numbers are 1567, 1657, 1675, 5176, etc., as long as the first digit is 5,6,7. For example, 1567: sum 1+5+6+7=19, product 1×5×6×7=210. So 19×210=3990. Therefore, this works.Wait, but before jumping to conclusion, let me verify. So if the number is 1567, sum is 1+5+6+7=19. Product is 1×5×6×7=210. Then 19×210=3990. Yes, that's correct. So 1567 is a valid solution. Are there others?But the problem says "Find at least one four-digit number", so we need at least one. However, maybe there are others. Let's check if there's another combination for S=19, P=210. For example, 3,5,7,2: sum is 3+5+7+2=17. Not 19. If we try combining more factors: 210=2×3×5×7. If we combine 2 and 3 to make 6, then we have 6,5,7,1. If we combine 2 and 5 to make 10, but 10 is not a digit. Similarly, combining 3 and 5=15, which is not a digit. So the only way is 1,5,6,7. Hence, the four-digit numbers are permutations starting with 5,6,7, or 1, but since it's four-digit, starting with 1 is allowed (wait, no: four-digit numbers can't start with 0, but starting with 1 is allowed). Wait, 1567 is a four-digit number. So numbers starting with 1 are allowed, such as 1567, 1657, 1675, 5167, etc. So there are multiple numbers here.But the problem asks for at least one, so 1567 is a valid answer. However, let's check other pairs just to see if there are other possibilities.Continuing with S=21, P=190:190=2×5×19. Again, 19 is too big. So impossible.S=30, P=133:133=7×19. Again, 19 is too big. So impossible.S=35, P=114:114=2×3×19. Again, 19 is too big. So impossible.Therefore, the only feasible pair is S=19 and P=210, which gives us numbers like 1567.But wait, let's just confirm once again. Let's take 1567:Sum: 1+5+6+7=19Product:1×5×6×7=21019×210=3990. Correct.But also, are there other combinations for S=19 and P=210? Let's see. For example, if we use digits 2, 3, 5, 9. Sum:2+3+5+9=19. Product:2×3×5×9=270 ≠210. So not good. What about 3, 5, 5, 6: sum 3+5+5+6=19. Product:3×5×5×6=450 ≠210. Not valid.Another combination: 4, 5, 5, 5: sum=19? 4+5+5+5=19. Product=4×5×5×5=500 ≠210. Nope.Alternatively, 2, 2, 7, 8: sum=2+2+7+8=19. Product=2×2×7×8=224 ≠210.Hmm. What about 3, 2, 7, 7: sum=3+2+7+7=19. Product=3×2×7×7=294 ≠210.Alternatively, 1, 5, 6,7 as before. So that seems unique. Because 210=1×5×6×7. So the digits have to include 1,5,6,7. Any other combination would require different factors, but 210's prime factors are 2,3,5,7. So if we arrange these into four digits (with 1 allowed), the only way is 1,5,6,7. Because 2×3=6, and then 5,7,1. So that's the only combination. So the four-digit numbers are permutations of 1,5,6,7, with the first digit not being 0, which it isn't in any case.Therefore, possible numbers include 1567, 1576, 1657, 1675, 1756, 1765, 5176, 5197, etc. Wait, but 5197 would be 5,1,9,7. Wait, hold on: the digits have to be 1,5,6,7. So any permutation of those four digits. So numbers like 5176, 5716, 6157, etc. So all permutations where the digits are 1,5,6,7. So there are 4! =24 permutations, but since the first digit can't be zero, but all digits are 1,5,6,7, none of which are zero, so all 24 permutations are valid four-digit numbers. Therefore, there are 24 numbers that satisfy the condition. Examples include 1567, 1657, 5167, 6157, etc.But the problem says "Find at least one four-digit number", so we can list one of them, such as 1567.Wait, just to be thorough, let me check another permutation. Let's take 5176:Sum:5+1+7+6=19Product:5×1×7×6=21019×210=3990. Correct.Another one: 6517:6+5+1+7=19, product=6×5×1×7=210. Correct.So, indeed, all permutations work.Therefore, the answer is any four-digit number composed of digits 1,5,6,7. The problem asks for at least one, so 1567 is a valid answer. However, let's check if there are other possible combinations outside of S=19 and P=210. Wait, we went through all factor pairs and only S=19 and P=210 worked. So that's the only solution.But just to be 100% sure, let's see if there's another way to get S=19 and P=210 with different digits. Wait, we considered 1,5,6,7. Is there another set of four digits that sum to 19 and multiply to 210?Let's try to think differently. Suppose we have four digits a,b,c,d. Their sum is 19, product is 210. Let's see if there are other possibilities.We know 210 factors into 2×3×5×7. So, the digits have to be these primes or products of these primes. Since each digit must be between 1 and 9, the possible digits are the factors of 210 in that range. The factors of 210 are 1,2,3,5,6,7,10,14,15,21,30,35,42,70,105,210. But digits can only be up to 9, so possible digits are 1,2,3,5,6,7.So, the digits have to be selected from 1,2,3,5,6,7. We need four of them (with repetition allowed?) Wait, repetition is allowed, but in the factorization 2×3×5×7, all are distinct. If repetition is allowed, perhaps we can have duplicates.Wait, but 210=2×3×5×7. If we want to have four digits, possibly combining some factors. For example:If we take 2×3=6, then 6,5,7,1. This gives the digits 1,5,6,7.Alternatively, 2×5=10, but 10 is not a digit. Similarly, 3×5=15, which is not a digit. So the only possible way to break down 210 into four digits is 1,5,6,7. So there's no other combination.If repetition is allowed, like using 1 multiple times, but even then, the product would still need to be 210. For example, 1,1,5,42: but 42 is too big. 1,1,6,35: 35 too big. So no, repetition doesn't help here. Therefore, the only possible digits are 1,5,6,7. Hence, the only four-digit numbers are permutations of these digits.Therefore, the answer is 1567 (or any permutation of these digits, but 1567 is the smallest such number). So the final answer is 1567, but let me confirm once again:Sum:1+5+6+7=19Product:1×5×6×7=21019×210=3990. Perfect.Yes, that satisfies the condition. Therefore, the answer is 1567, and it's boxed as per instruction.Final Answerboxed{1567}</think>To find a four-digit number such that the product of the sum of its digits and the product of its digits equals 3990, we start by denoting the number as (ABCD) where (A, B, C, D) are its digits. We need ( (A + B + C + D) times (A times B times C times D) = 3990 ).First, we factorize 3990:[ 3990 = 2 times 3 times 5 times 7 times 19 ]Next, we consider the possible values for the sum (S = A + B + C + D) and the product (P = A times B times C times D) such that (S times P = 3990). We list the factor pairs ((S, P)) where (4 leq S leq 36) and (111 leq P leq 997.5):- Possible pairs: ((5, 798)), ((6, 665)), ((7, 570)), ((10, 399)), ((14, 285)), ((15, 266)), ((19, 210)), ((21, 190)), ((30, 133)), ((35, 114))We check each pair to see if there exist four digits (1-9) that sum to (S) and multiply to (P):- For (S = 19) and (P = 210): - The product (210) factors into (2 times 3 times 5 times 7), which can be combined as digits (1, 5, 6, 7) (since (2 times 3 = 6)). - The sum of these digits is (1 + 5 + 6 + 7 = 19).Thus, the digits (1, 5, 6, 7) form valid four-digit numbers. Permutations of these digits include numbers like 1567, 1657, 5167, etc. Verification:- For the number 1567: - Sum: (1 + 5 + 6 + 7 = 19) - Product: (1 times 5 times 6 times 7 = 210) - Result: (19 times 210 = 3990)Therefore, the four-digit number is (boxed{1567}).]
🔑:Solution. Note that 3990=2 cdot 3 cdot 5 cdot 7 cdot 19=1 cdot 6 cdot 5 cdot 7 cdot 19 and 6+5+7+1=19. Therefore, any four-digit number that contains one 1, one 6, one 5, and one 7 will work, for example, 1567.Comment. To receive full credit, it is sufficient to provide any correct example.